
Introduction
Evolving healthcare needs in this post-COVID era have led to ongoing challenges in delivering quality medical care. Persistent worker shortages and higher patient volumes contribute to bed availability issues in hospitals, which in turn result in overcrowding in emergency rooms.1 Care coordination and efficient discharge planning are also difficult due to suboptimal communication between healthcare staff and the high complexity of patients’ needs.2 Collectively, these factors reduce throughput across the hospitals, compromise the quality of care, and heighten patient dissatisfaction and boarding in emergency rooms.3
In response to concerns about the US healthcare systems’ underperformance in safety and quality metrics, various approaches have been explored to optimize care coordination and discharge planning for hospitalized patients. One such approach is the implementation of accountable care team models in inpatient hospital units across the country. These models emphasize cost of care and inter-professional collaboration and have demonstrated improvements in data-driven decision-making.4 Physicians traditionally accustomed to making independent medical care decisions are increasingly engaging in inter-professional multidisciplinary collaboration to provide high-quality care.5
The cornerstone of this collaboration is interdisciplinary rounds, which engage various team members (physicians, nurses, case management, social workers, physical therapists, and pharmacists) in addressing patients’ needs and discharge planning, thus affecting hospitals’ throughput. Healthcare systems dedicate significant efforts to defining the exact roles of various team members within these rounds. The significance of clinical nurse leaders in facilitating interdisciplinary collaboration has already been recognized.5 Some hospitals also include skilled nursing facility (SNF) liaisons in interdisciplinary rounding, which has been shown to reduce the length of stay for complex medical patients.6 Interdisciplinary rounds are ever evolving and improving and are crucial to inpatient medical care.
In line with hospitals nationwide, our healthcare system has recognized the need for enhanced interdisciplinary communication, improved care coordination, and overall patient experience. With a focus on improving throughput and fostering a more effective frontline team through improving our interdisciplinary rounds model, we addressed several challenges in the current rounds’ structure. These included insufficient attention to discharge planning, unstructured, time-consuming rounds, lack of closed-loop communication, and ambiguous ownership of discharge barriers. While our institution, Evanston Hospital at Endeavor Health, has been meeting our metric goal for length of stay (LOS), we still struggled with hospital throughput and emergency room boarding time. Thus, early discharges remained a priority. Our objective was to develop rounds focused on improving throughput by accurately identifying the estimated date of discharge (EDD), understanding, and addressing discharge barriers, and improving median discharge time. Our secondary objective was to ensure that rounds were efficient, with pertinent exchange of information, with hopes of resulting in improved patient experience.
Methods
We utilized the Institute for Healthcare Improvement (IHI) Plan-Do-Study-Act (PDSA) Model to achieve our objectives.7 The pilot was implemented on a 33-bed adult general medicine non-teaching unit in Evanston Hospital, Endeavor Health. Most patients in our pilot unit are distributed between two hospitalist services, with an average of five patients in gynecology-oncology and urology services. During the implementation of our pilot, a total of five hospitalists rounded on that unit. The majority of our patients are hospitalized for sepsis, heart failure, pneumonia, liver failure, kidney failure, and alcohol withdrawal. We chose this unit based on its historical record of below-target patient communication scores, difficulties with discharge coordination, and the wide range of diagnoses.
Our project consisted of four distinct PDSA cycles and engaged the essential stakeholders: nursing leadership, pharmacy, case management (CM), physical therapy (PT), hospitalist leadership, and inpatient acute care quality leadership. We aimed to improve EDD identification (the percentage of patients discharged on the same day as identified), median discharge time, and patient experience scores (as illustrated by Press Ganey Scores). Balancing measures included the time spent in rounds and the number of secure chats and pages after rounds. Stakeholders had weekly meetings to discuss process improvement, barriers observed by team representatives, and the next steps.
Our first PDSA cycle lasted one week. In this cycle, all frontline team members - physician, nurse, CM, PT, and pharmacist were present in rounds at the same time. In order to prioritize discharge planning and the throughput, the initial intervention was a physician-led discussion focusing on identifying the EDD for each patient. Rounds would focus on patients anticipated to be discharged the same and the following day and on identifying discharge barriers. We quickly realized that this was ineffective for multiple reasons: lack of space with a large number of team members in rounds, disruption/fragmentation of rounds for nursing (nurses needed to leave the room several times as rounds were physician-led), and extended time in rounds (>1 hour).
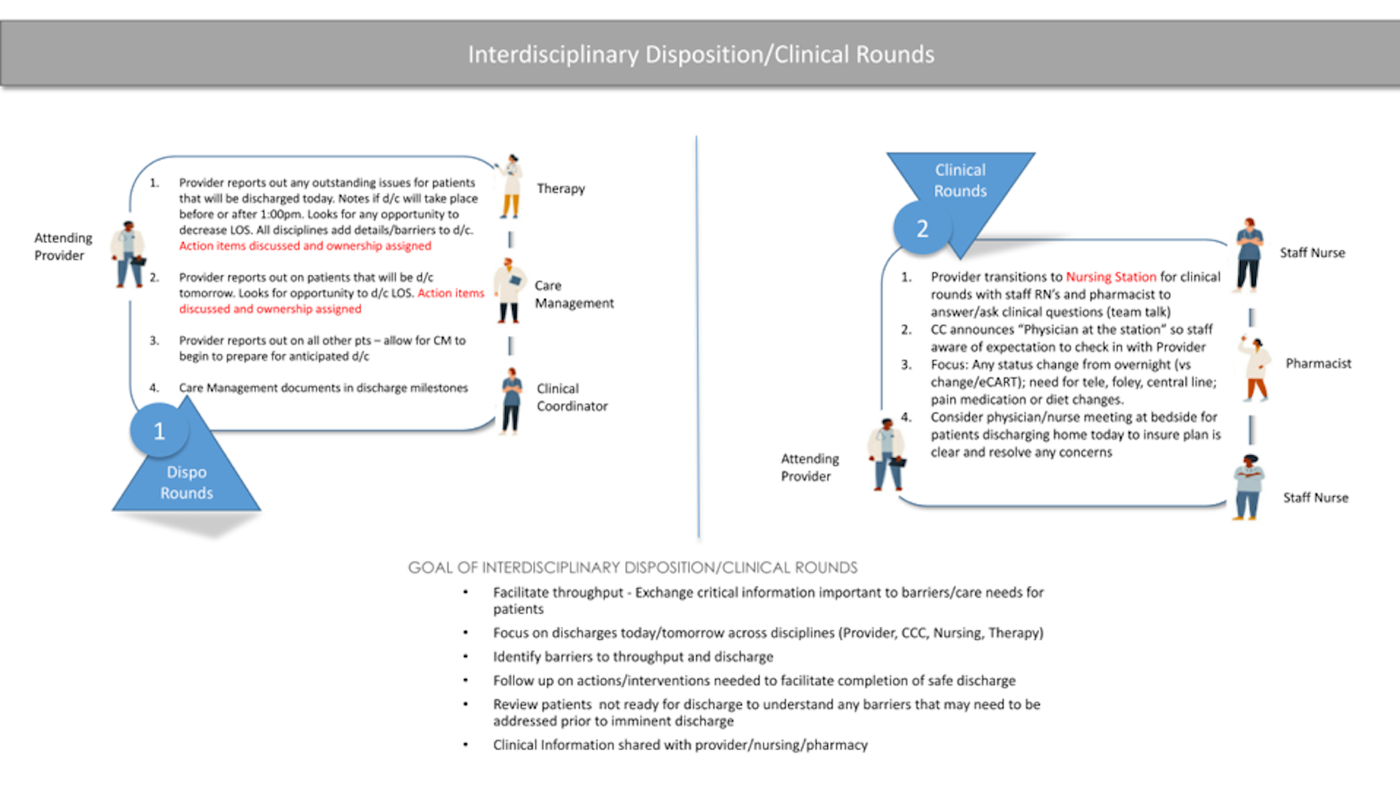
In our second PDSA cycle, it was decided to split the rounds to interdisciplinary disposition and clinical rounds (Figure 1). Interdisciplinary disposition rounds included the physician, nursing coordinator, physical therapist, and case management. The focus remained on EDD and discharge barriers for patients anticipated to be discharged the same or the following day. Each identified barrier was assigned to a specific team member responsible for addressing it by the end of the day. For example, CM was to expedite the arrangement of home health services or skilled nursing facility placement for patients to be discharged the same and the following day, or PT was asked to prioritize assessing patients nearing discharge pending PT evaluation. An additional discussion point added in PDSA cycle 2 was an arrangement of transportation to the discharge destination a day prior to discharge. The physician would determine the approximate discharge time for the next day, and nursing managers and CM would arrange the mode of transportation.

The second part of the interdisciplinary rounds consisted of clinical rounds. This was attended by the physician (after completing disposition rounds), bedside nurses, and the pharmacist. During this time, clinical patient care information was exchanged. Our second PDSA cycle lasted two weeks.
A third PDSA cycle was prompted by the observation that team members did not focus on exchanging pertinent patient care information during the clinical rounds (such as the presence of a Foley or central line, telemetry usage, and DVT prophylaxis). To ensure that the clinical team discussion has an appropriate framework and that key patient safety indicators (PSI) are being captured, we created the Safety Board - an EPIC (our electronic medical record) generated list (Figure 2). The physician accesses the Safety Board on the computer during the clinical rounds and reviews each item of the Safety Board with the nurse and pharmacist, ensuring that all the elements are being addressed. The teams were asked to remove central lines and Foley catheters if deemed unnecessary promptly, address resource overutilization (such as telemetry), and ensure patient safety (DVT prophylaxis).
This third PDSA cycle lasted for two months. During this time, we coached our team members to use the Safety Board and exchange only relevant information. Teams were encouraged to follow scripted elements closely; if further discussion was needed, they were to be held outside of the structured rounds to ensure timeliness and efficiency. Teams were instructed to follow the script for disposition rounds, as demonstrated in Figure 1. For clinical rounds, teams were instructed to review each patient’s Safety Board (Figure 2) and not extend discussion beyond this for time and efficiency purposes.
-generated_list_that_pulls_in_patient_safety_indicator_(ps.png)
Despite restructuring the interdisciplinary rounds and streamlining team communication, we did not observe a significant improvement in patient experience scores. This led to the fourth and final PDSA cycle, which introduced an additional intervention for physicians to perform second rounds on patients planned for discharge that same day. The second rounding reinforced discharge medications and post-discharge follow-ups, allowing patients and their families to ask questions. An analysis of the patient experience scores showed that scores were the lowest among patients older than 75 who were discharged home. Thus, our intervention focused on this group, with frontline physicians in charge of identifying this patient population and conducting second rounds after attending interdisciplinary rounds.
The fourth PDSA cycle lasted three months, and we closely followed the patient experience scores. After this final intervention, we felt that our rounds were optimized, so our weekly meetings with the stakeholders ended as no further adjustments were needed. However, we continue to follow up on interdisciplinary rounds metrics and compliance during our monthly pavilion leadership meetings.
Results
The LOS metric was met at our institution, and thus our focus was on earlier discharges to help with hospital throughput. In our unit, we achieved a reduction in median discharge time of 1 hour and 10 minutes; specifically median discharge time was previously 3:25 p.m. and moved to an earlier time of 2:15 p.m. with redesigned interdisciplinary rounds. This was attributed to proactively addressing discharge barriers and arranging transportation to discharge location a day ahead of discharge.
Prior to the implementation of the rounds redesign, the EDD accuracy was 66%. After interdisciplinary split rounds were introduced, greater than 80% of patients were discharged on the day identified. We attributed this improvement to the structure of the interdisciplinary rounds and continuous discussion about EDD.
To ensure appropriate time use for our team members, during the early stages of this redesign our administration team monitored the duration and content of clinical and disposition rounds. Depending on patient census (ranging usually from 12-15), each section of rounds ranged from 10-12 minutes. In comparison, in our old iteration of rounds, which were less scripted and without clear direction, rounds lasted approximately 25-30 minutes per physician team. With restructured rounds, total physician time in rounds was modestly reduced by 5-10 minutes. However, the time spent in rounds was reduced substantially for our multidisciplinary teams (CM, nursing, PT and pharmacy), with an average reduction of 15 minutes.
With the split rounds, there were occasional gaps observed in information exchange between the nursing staff and case management (for example - a change in patient’s discharge preference that was conveyed to nursing but not to the physician and CM team). To address this challenge, the floor nursing leaders served as liaisons between nursing and CM. They collected pertinent discharge-related information from the nurse prior to disposition rounds, and shared discharge plans conveyed from CM to the nurses after clinical rounds.
Our additional balancing measure was a number of messages via our electronic health record (secure chats) and pages going out to our physicians. We encountered limitations in tracking the precise number of secure chats and pages within our EPIC system, thus had to rely on anecdotal feedback from our physicians. All five physicians rounding on our pilot unit reported a decrease in the volume of secure chats and pages. We attributed this to pertinent scripted information being addressed in rounds- physicians were not paged or secure-chatted on items already addressed with the safety board, such as discontinuing telemetry, Foley catheters, and diet orders. Additionally, we observed anecdotal improvements in camaraderie and collaboration among different disciplines, enhanced ownership of unit needs, and comprehensive discharge planning.
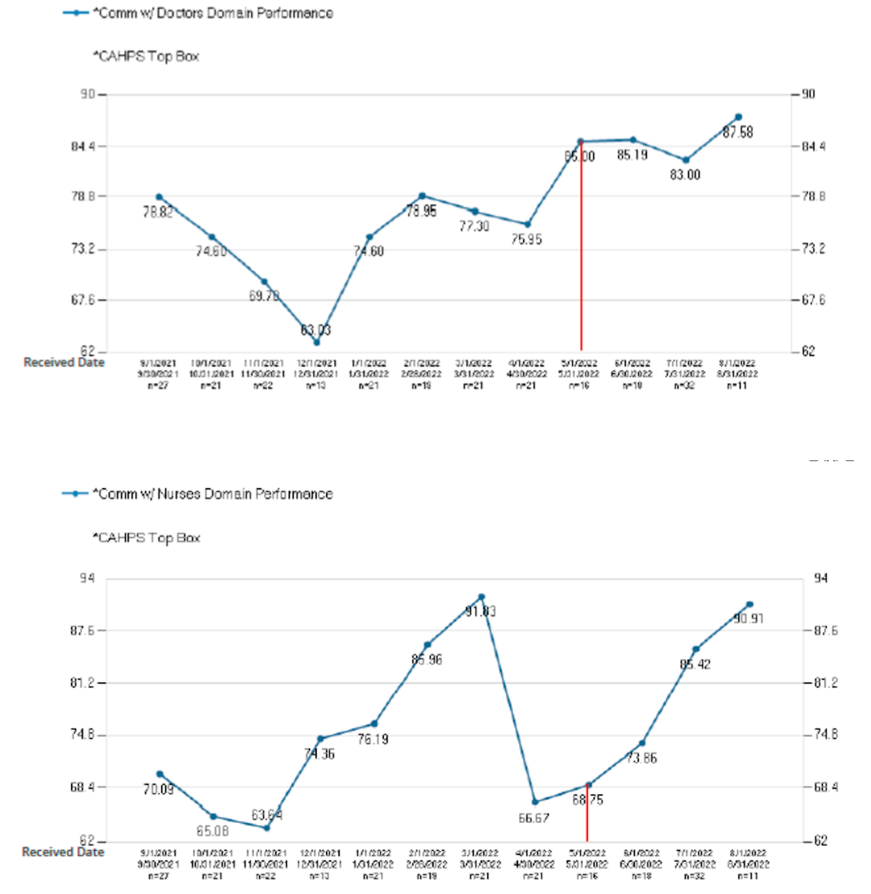
Second physician rounds on discharging patients resulted in significant improvement of patient experience (PEX) scores as illustrated in figure 3. Along with efficient discharge, PEX was a major driver of our intervention and a priority for our institution. In the months preceding our pilot, there was a significant decrease in patient experience scores, likely in part due to the second COVID surge. We also observed a significant decrease in nursing communication scores in April 2022; this was attributed to high nursing turnover and significant nursing shortage at our institution.

Physicians conducted second rounds after seeing all of their patients and after interdisciplinary rounds. It is important to note that due to the improved effectiveness of interdisciplinary rounds, which addressed most of the pertinent patient care information, and with anecdotally reduced paging and messaging from the nursing and CM team, physicians had time to perform second rounds. During those rounds, physicians could focus exclusively on discussing discharge instructions with the patients and their families. The positive trend in PEX scores is noted in physician and nursing communication domains. Importantly, second rounds did not negatively affect early discharges.
Discussion
Interdisciplinary rounds are vital in enhancing patient care coordination by engaging diverse team members collaboratively. Despite their importance, our institution, like many others, faces limitations with the effectiveness of rounds. These challenges frequently stemmed from divergent priorities among team members, resulting in suboptimal participation. Physicians and nurses emphasize and focus on medical needs, whereas case management prioritizes safe and timely discharge planning.8 Additionally, rounds often suffer from the exchange of irrelevant information, inefficiency, and uncertainty about task ownership.9 Streamlining effective and clear communication for multidisciplinary teams becomes essential to achieve smooth patient care coordination.10 With our rounds redesign, we achieved better identification of EDD, improved median discharge time, reduced time spent in rounds, and improved patient communication in the pilot unit.
Accurate determination of EDD remains a hospital priority, as it helps optimize the throughput of hospitalized patients, facilitates the transition of care, and communicates discharge date expectations clearly by all team members to the patients and their families. Early EDD prediction upon hospitalization is only accurate for 22% of patients.11,12 With a focus on discharge planning during our disposition rounds, we achieved greater precision in identifying and adhering to EDD, improved identification of discharge barriers, timely transportation arrangement, and improved median discharge time. Median discharge time was notably not negatively impacted by the second physician rounds. While existing literature suggests that earlier discharges do not enhance throughput, our achievements proved particularly useful during the COVID surge, where we had prolonged emergency department boarding times and significant nursing shortages.12 Early discharges helped set expectations about in-hospital bed availability and anticipated discharge times (such as when transport was coming).
Al Halabi et al. indicated that physicians, managing an average of 14 patients, spend a median of 14 minutes per patient encounter in the inpatient setting in their 11-hour work day.13 Furthermore, physicians dedicate approximately 3.8 hours (±2) daily, constituting about 37% (±17%) of total work hours, to electronic health record (EHR) activities.14 Nurses face similar challenges, with greater time allocated to indirect care than direct patient interaction.15 Ensuring productive interdisciplinary rounds was necessary, given the time limitations faced by frontline staff.
Our literature search did not reveal a comparable interdisciplinary round structure in other US hospitals. By splitting rounds in our institution, we reduced the time nurses, PT, CM, pharmacy, and physicians spent in rounds. Adhering to the scripted rounds ensured efficient exchange of pertinent information, leading to fewer interruptions (like secure chats and paging) and affording more time for direct patient care. This approach fostered team camaraderie, improved interdisciplinary communication, and enhanced patients’ perception of a unified team. Effective communication enabled the implementation of second physician rounds for discharging patients, significantly improving patient experience as reflected in Press Ganey Scores across physician and nursing communication domains.
One of the limitations of this study would be the specific setting selected for initial implementation. It was conducted on a single unit in a tertiary care center with no resident staffing. Variations in patient populations, such as predominantly surgical patients or resident-covered units, may lead to challenges in implementing some of the interventions. Another limitation is that geographic cohorting (where physicians are assigned to a single unit) is necessary for the split rounds to be successful. For hospitals with no geographical cohorts, splitting the rounds will be challenging to implement, and the benefits described may not be achievable. The third limitation was the inability to accurately track the number of secure chats and pages due to EPIC EHR limitations and the need to rely on anecdotal data from our frontline team. The fourth limitation was that nursing occasionally missed essential discharge information from the disposition rounds. We did mitigate this with the nursing coordinator communicating discharge plans with nursing after the rounds. Finally, second physician rounds may be observed as additional work for busy clinicians. We assured buy-in by illustrating improved patient care communication, reduced number of pages, secure chats, and time spent in rounds.
Moving forward, we plan to implement split interdisciplinary rounds in other units in our hospital and in four other pavilions in Endeavor Health. These units have differing patient populations: oncologic, cardiac, surgical, and orthopedic patients. We hope to gather similar results regarding improved EDD identification, median discharge time, and patient experience. However, we also recognize the need to conduct PDSA cycles and adjust the structure to meet each unit’s individual needs.
For hospitals interested in implementing our intervention, we acknowledge that splitting rounds into two parts can initially seem counterintuitive and redundant. We suggest closely following our rounds model as illustrated in Figure 1. Awareness of EDD, implementation of transportation discussions in interdisciplinary rounds, and focus on discharge planning for patients with EDDs set for today or tomorrow will help improve discharge time. We also suggest implementing the Safety Board (or a similar EHR-generated guide) to streamline clinical conversation between physicians, nurses, and pharmacies and improve the identification of resource utilization. To assure frontline team buy-in, strong leadership support is needed.
In summary, we recommend our approach of split interdisciplinary rounds given positive results on patient experience, improvement of EDD, streamlined discharges, and bringing key patient safety indicators to the forefront of the clinical conversation.
Acknowledgments
We would like to acknowledge whole staff of 4Louis at Endeavor Health, Evanston Hospital, led by Ruth Jordan, RN and Stephanie Mills, RN, for the contributions in implementing this initiative.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest.
Corresponding author:
Marina Kovacevic, MD
Hospitalist, Endeavor Health
Clinical Assistant Professor, University of Chicago, Pritzker School of Medicine
2650 Ridge Ave, 4th floor, room 4206, Evanston, IL, 60201
Email: mkovacevic@northshore.org
Ph: 847-532-2638