Introduction
Healthcare costs have become increasingly concentrated among a subset of patients: 1% of patients account for 22.7% of healthcare spending.1 By contrast, the bottom half of the population account for just 2.7% of healthcare spending.1 More than a third of American healthcare spending goes to hospitals.2 Efforts aimed at reducing healthcare expenditures have focused on limiting hospital admissions and reducing length of stay. Every year, there are more than 35 million unique hospital stays in the United States, with 6.7% of Americans admitted to the hospital at least once.3
Surprisingly, there has been limited research characterizing patients with prolonged hospitalizations. We describe this population in order to help anticipate patients at risk for requiring extended hospitalizations of at least six months. We present a retrospective analysis of admission diagnoses, common medical complications, sociodemographic information, and barriers to discharge with an emphasis on modifiable risk factors of this patient population.
Methods
This study was approved by the Institutional Review Board at the University of Florida College of Medicine. We performed a retrospective analysis from January 1, 2012, to January 1, 2022, at University of Florida Health Shands Hospital (UFHSH). Adults with hospitalizations lasting longer than six months were identified using the UFHSH Integrated Data Repository. Patient data was collected from the electronic medical records system.
An Extensively Prolonged hospitalization (EPH) was defined as an admission to our medical center for an uninterrupted period of at least six-months (183 days). Patients awaiting solid organ transplant or admitted to the psychiatry unit at any point were excluded from the analysis.
Among 393,474 total adult hospitalizations, 73 were identified as having lasted longer than six months. Among the 73 patients, 29 were excluded because they were awaiting transplant (22 for heart transplant and 7 for lung transplants). Two patients were excluded because their stay was in the psychiatric hospital. Forty-two adult patients (0.01%) were included in the final analysis.
Patient data, including past medical history, reason for admission, hospital course, and outcome, were collected. Barrier to discharge was categorized as “unmet post-acute facility need” only if patients were stated to be “medically stable for discharge” for at least three months. A full waiver of informed consent and waiver of HIPAA privacy authorization for identifying and enrolling subjects was obtained under IRB approval. Statistical analysis included Chi-Square tests to analyze factors associated with medical decision-making incapacity. A 95% Confidence Interval and a p value of 0.05 were used to determine statistical significance. Statistical analysis was performed with SPSS 28.0.1.0 (142) (IBM Corp, Armonk, NY).
Results
Patient Characteristics
The characteristics of the study population are summarized in Table 1. The study cohort was 62% male with a median age was 58.5 years old (IQR 48.8-67.5; range: 21-80). Median BMI was 25.5 (range: 15.13-63.00). Twenty patients were Caucasian (48%) and 17 were African American (40%). The most common comorbidities were history of CVA (48%), COPD (21%) and congestive heart failure (17%). Three patients had private insurance while thirty-nine patients (93%) were insured by Medicare or Medicaid. Places of living prior to hospitalization included 22 patients (52%) living at home, 11 (26%) at a group-living facility, and 7 (17%) who arrived as transfers from outside hospitals. Thirteen (31%) patients were married and five (12%) had a history of homelessness.
Hospital Presentation
The most common presenting symptoms were neurological (11 patients; 26%) and trauma-related (9 patients; 21%). Specifically, the most common symptoms on presentation were altered mental status (7), sepsis (6), and burn (6). Three additional patients were admitted for a scheduled procedure. Thirty patients (73%) were admitted from the emergency department to a critical care unit.
Hospital Stay
Average length of stay for all hospital stays during the study period was 5.49 days. When hospitalizations that exceeded the 99th percentile were removed, average hospital stay was 5.21 days. Among patients with EPH, mean and median length of hospital stay was 335 and 281 days, respectively (IQR range 229-375 days; range: 189-1052 days) (Table 1). Total hospital days during this period were 2,046,065. Though they made up 42 patients studied accounted for 14,080 days (0.69%) of hospitalization days.
The most frequently recorded hospital complications were mechanical ventilation (37) tracheostomy placement (33), and gastrostomy tube placement (30). Other hospital complications included sacral ulcer (17), renal replacement therapy (15), and attempted cardiopulmonary resuscitation (12).
Patients had an average of 8.88 CT scans, including 3.74 CT scans of the head (range: 0-17), 2.50 of the chest (range: 0-10), and 2.64 of the abdomen and pelvis (range: 0-12). Patients received an average of 2.12 MRI scans (range: 0-31). Specifically, blood cultures were positive
for methicillin-resistant Staphylococcus aureus (MRSA) in 19 patients (45%), vancomycin-resistant Enterococcus in 13 patients (31%), carbapenem-resistant organisms (CRO) in 9 patients (21%), and extended spectrum beta-lactamase in 4 patients (10%). Thirty-four patients (81%) had blood cultures result positive for at least one of these organisms at some point during their hospital stay. Palliative care was consulted for 26 patients (62%) while social work was consulted for 37 patients (88%).
Twenty-seven patients (64%) were considered stable for discharge with an unmet post-acute facility need at least three months. The main barrier to discharge was acute medical care necessity in 8 patients (19%) and unknown in 7 patients (17%). Patients had an unmet post-acute facility need at least three months were more likely to have a history of stroke (63% vs. 21%; p = 0.012), to have a social work consult (100% vs. 66.7%; p = 0.001), and to be deemed incapacitated, (p = < 0.001); they were less likely to pursue palliative care (3.7% vs. 60%; p = <0.001). There were no statistically significant differences in blood culture positivity, length of stay, or overall survival.
Medical decision-making
Eight patients (19%) were deemed capacitated to make medical decisions at any point during hospitalization while 34 patients (81%) were deemed incapacitated. Of the 34 incapacitated patients, 0 had an advanced directive documented or an appointed healthcare surrogate. Health care surrogate(s) were most frequently adult child (15), spouses (11), parents (4), sibling (3), court-appointed guardian (3). Seven patients had multiple (≥ 2) decision makers, including one patient with 20 adult children who had equal weight in medical decision-making. Compared to patients who deemed capacitated, incapacitated patients were more likely to have public insurance (84.6% vs. 15.4%, p = 0.029), to have been ready for discharge for at least 3 months (96.3% vs. 3.7%, p = <0.0001), to have placement listed as the main barrier to discharge (96.3% vs. 3.7%, p = <0.0001 ), and to have a social work consult placed (89.2% vs. 10.8%; p = <0.0001).
Outcomes
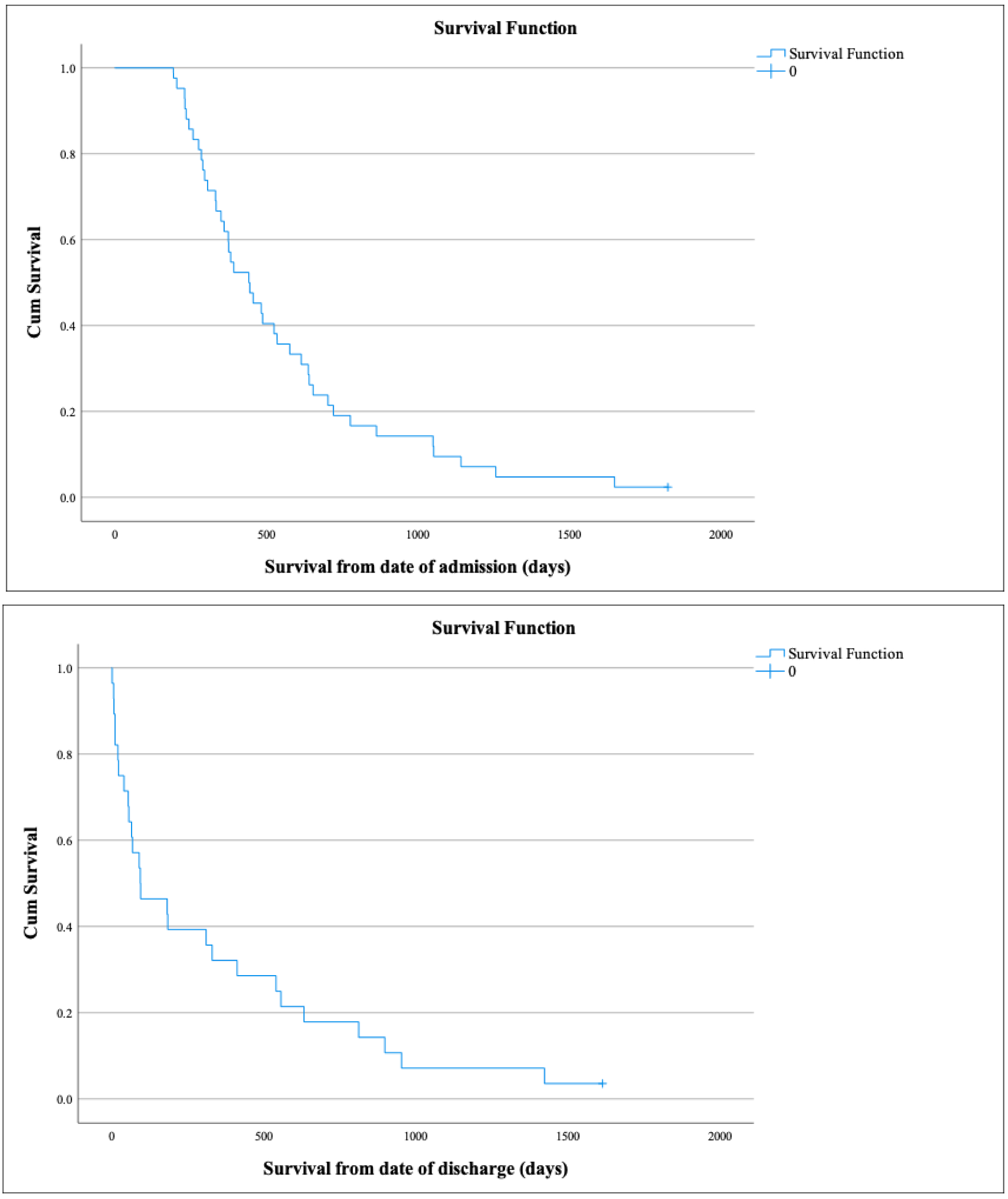
Median overall survival from start of hospitalization was 442 days ± 58 days. Thirteen patients (31%) died in the hospital; 5 died despite receiving CPR and 8 died with “do not resuscitate” orders in place. Twenty-nine patients (69%) survived to discharge. Kaplan-Meyer plots are provided below (Figure 1). Among the 29 patients who were discharged from the hospital, 23 went to a group-living facility (including subacute nursing facilities and rehabilitation facilities), 3 patients went to hospice facilities, and 3 patients went home with home nursing ordered. Median survival for discharged patients was 94 days.

Two patients were lost to follow-up after leaving the hospital. At follow-up three years since admission date, 3 patients (7%) were confirmed to be still alive. Five years after admission, one patient (2%) was still alive. Of the 3 patients who were still alive three years after admission, none were capable of living independently. Two of the patients were bedbound with severe neurocognitive impairment. One patient was ambulatory and was readmitted several times for self-neglect. This was the only patient confirmed to be alive five years after admission.
Hospitalizations Lasting Longer Than One Year
Eleven patients had hospitalizations lasting longer than one year. With a mean of 483 days, these 11 patients accounted for 6,034 hospital days (42% of the days accounted for by this cohort). With an average LOS 92 times the average, these 11 patients made up 0.00053% of all patients admitted during the studied time and 0.30% of all admission days. The longest hospital stay was 1052 days. Nine of the 11 patients were unable to make medical decisions for themselves at any point during their admission. Patients were considered stable for discharge for at least three months in all but one case. Five patients died during the hospitalization. Six patients were discharged; one was immediately lost to follow-up and five patients died 22, 40, 54, 56, and 94 days after discharge, respectively. One patient had private insurance and 10 had Medicare or Medicaid (Table 2).
DISCUSSION
The average length of stay in American hospitals is about 5.2 days, though the range is broad.3 At the tail end of the curve are patients that stay in the acute hospital setting for greater than six months. We present a retrospective analysis of patients with EPH performed at a large, public tertiary care center in Florida with a catchment area that includes both rural and urban areas. To the best of our knowledge, this is the first study to describe EPH.
Although EPH made up an extremely small percentage of all admissions, they accounted for a significant number of hospital days. With a combined 14,080 hospital days (38 years, 210 days), the 42 admissions accounted for 0.01% of hospital admissions and 0.69% of hospital days. Surprisingly, there has been limited research characterizing prolonged hospitalizations (PH), and studies that have analyzed prolonged hospitalization have used thresholds of 14 to 30 days.3–6 In analyses PH lasting at least 21 days on an internal medicine service at a Colorado hospital, PH was found to be associated with MRSA bacteremia (2%), palliative care consult (15%), ICU stay (59%), and public insurance (Medicare and Medicaid).6 Two analyses of post-surgical patients also found associations of PH with public insurance.7,8 In our cohort, all but 3 patients had public insurance. In a separate study of PH among patients admitted through the emergency department, cognitive impairment was found to be independently associated with prolonged hospitalization among patients admitted through the emergency department.[9] In our cohort, 81% of patients were cognitively impaired.
The main barrier to discharge in our cohort was an unmet need for post-acute facility bed, which was the case for at least three months for 27 patients (64%). In contrast, only 8 patients (19%) had a medical need requiring ongoing hospitalization for acute care as their primary barrier to discharge. In-hospital waiting for discharge is linked to a number of adverse outcomes and is independently associated with increased mortality.9,10
In a study of geriatric patients with PH ≥ 20, the primary barrier to discharge was medical necessity for inpatient stay in 55% of cases and difficulty coordinating discharge to subacute nursing or rehab facility in 22% of cases.11 In a study of VA patients, meanwhile, post-acute care facility needs were the most common cause of extended hospitalization.12 Difficulties in finding an adequate post-acute care bed were often multifactorial, including complex medical needs such as requirement for ventilator management, requirement of treatment for multi-drug resistant organisms requiring isolation, outstanding bills, lack of adequate insurance, and criminal record.12 EPH were associated with poor outcomes. Thirteen patients died in the hospital. Of the 29 patients who survived their hospitalization, 26 were discharged to a facility and 3 were discharged home with home nursing care. Strikingly, median post-discharge survival was just 94 days. Two patients were immediately lost to follow-up. Among the 27 patients, 26 had died within 5 years. None of the patients who were discharged were ever able to live independently.
There was a paucity of advanced care planning among patients with EPH. Only 1 of the 42 patients completed an advanced directive or designated a healthcare surrogate. These medical documents are important for guiding care when patients are medically incapacitated.13,14Capacity to make medical decisions is defined as the ability of a patient to understand the risks and benefits of an intervention and to understand the alternatives.13 When patients are incapacitated to make decisions, advanced directives are used to help a surrogate is responsible for making decisions on behalf of the patient.
The lack of advanced care planning meant that many patients had medical decisions made for them by the legal default healthcare proxy. Of the 42 patients included, 34 were deemed to be incapacitated to make medical decisions throughout their hospitalization. None of these patients had completed an advanced directive or designated a healthcare surrogate, so default healthcare proxy was used in each case. In the state of Florida, the order of proxy is as follows: spouse, adult child, parent, sibling, adult relative, or close friend.15 When no suitable proxy can be found, as was the case for three patients, a court-appointed proxy is used. The 34 incapacitated patients received many procedures, including gastrostomy-tube placement, tracheostomy tube placement, and cardiopulmonary resuscitation that we cannot know if they would have consented for. While surrogates are encouraged to make decisions on behalf of the patient’s best interest, several studies have shown that there is often discordance.16 These findings stress the importance of advanced care planning.
There are no case series on patients with hospitalizations lasting longer than one year. In our cohort, there were 11 such patients. Making up 0.00053% of all hospital admissions, the 11 patients with PH exceeding one year accounted for 0.3% of all hospital days. Of the 11 patients, just two were deemed capacitated to make medical decisions for themselves at any point during their admission. Most of the patients had long-term neurocognitive impairment; 4 patients had severe dementia and 4 had suffered a CVA. Of the 6 patients who survived to discharge one was immediately lost to follow-up and the other 5 died within the next 94 days.
Caution should be used in interpreting our findings, as the cohort was quite small and there was no comparison group. Factors that appear to stand out, such as the high rate of medical incapacity, may be unique to our cohort and not associated with EPH. Additionally, our cohort was included patients from 2012 to 2022. While this group was treated homogenously, changes in access to healthcare, availability of nursing home beds, and many other factors undoubtedly changed during this period and are continuing to change.
In our cohort, no patient with an EPH survived to live independently, and just one was alive after five years. Long-term were extremely poor. Larger studies are needed to further investigate these poor outcomes, which could play an important role in helping patients and families decide whether to undergo invasive procedures and to assist healthcare providers in goals of care discussions.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest
Corresponding author:
Ellery Altshuler, MD
Department of Internal Medicine
University of Florida
1600 Archer Road, Gainesville, Florida 32608
Ellery.Maya-Altshuler@medicine.ufl.edu
(305) 389-6231