
A 61-year-old woman with a history of stage II pancreatic neuroendocrine tumor, left temporal meningioma, renal cell carcinoma (post-nephrectomy), percutaneous endoscopic gastrostomy tube dependence, deep vein thrombosis, and type II diabetes mellitus, presented to hospital with hyperglycemia. Her symptoms included increased thirst, frequent urination, and somnolence. On arrival, her vital signs were within normal limits. On the physical exam, lower abdominal wall tenderness was noted. Laboratory testing included a serum blood glucose of 554 mg/dL (ref: 70-115 mg/dL), alkaline phosphatase of 748 U/L (ref: 140-150 U/L), alanine aminotransferase of 1100 U/L (ref: 5-55 U/L), and aspartate aminotransferase of 694 U/L (ref: 5-34 U/L). Computed tomography (CT) of the abdomen and pelvis (AP) revealed a pancreatic mass causing a mass effect on the common bile duct. She underwent endoscopic retrograde cholangiopancreatography (ERCP) with biliary stent placement and percutaneous endoscopic gastrostomy (PEG) tube replacements during her hospitalization with discussions with surgical oncology for outpatient PET scans and treatment options (octreotide versus surgical intervention) for her pancreatic neuroendocrine tumor.
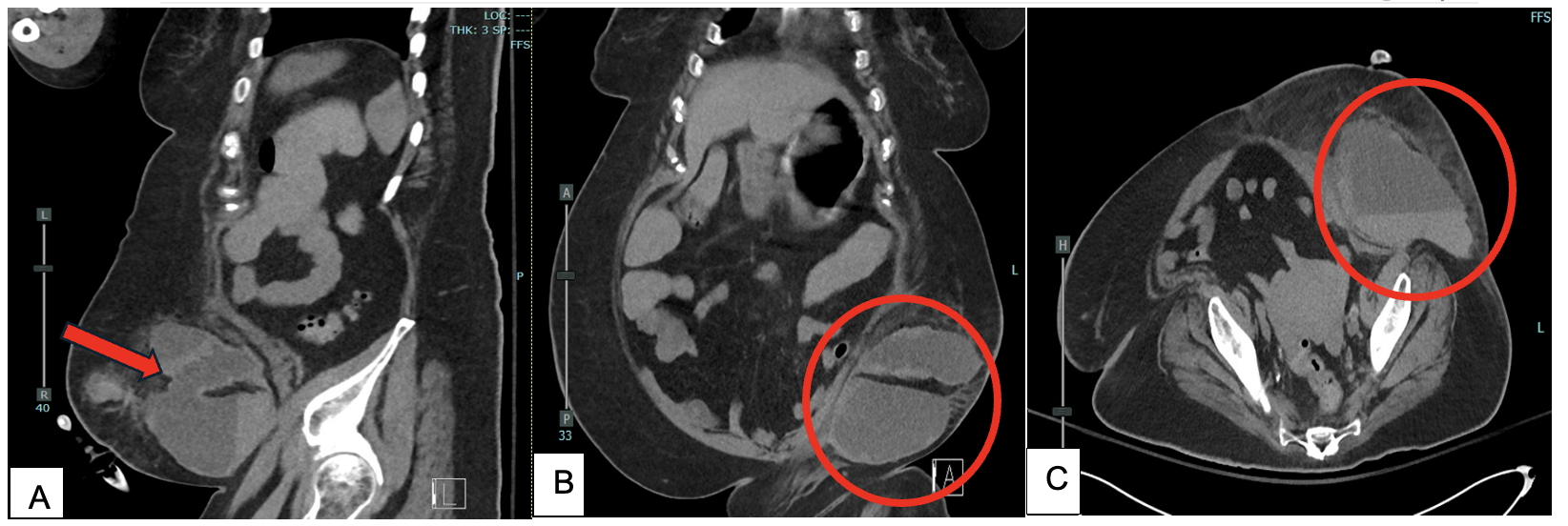
A few days later, she suddenly developed abdominal pain and sepsis with suspected acute mesenteric panniculitis and gastroparesis and remained in the hospital for several weeks for intravenous antibiotic treatment and stabilization. Physical examination revealed a large left-sided abdominal hematoma (Figure 1). She underwent another CT of the abdomen and pelvis that demonstrated a large hematoma (16 x 9 cm) with a hemoglobin drop from 8.1 to 6.6 g/dL (ref:11.9-15.8 g/dL), requiring 1 unit of transfusion (Figure 2). A repeat CT confirmed the hematoma with layering fluid. Of note, multiple new subcutaneous nodules superior to the hematoma were noted indicating possible areas of hemorrhage induced by metastatic lesions from her primary pancreatic neuroendocrine tumor. Interventional radiology embolized the left circumflex iliac artery. By hospital day 34, the hematoma had reduced in size, and she was discharged in stable condition with follow-up with surgical and medical oncology for treatment plans with octreotide.

_sagittal_view_of_abdominal_hematoma_measuring_16x9_cm_(red_arrow)._(b)_coronal_view_of.png)
Pancreatic neuroendocrine tumors (pNETs) are a rare disease with a prevalence of 25-30 per 100,000 population in the United States and an increased incidence over the last few decades from improved imaging technology.1,2 pNETs can be characterized based on their abilities to produce hormones such as insulinomas, gastrinomas, and glucagonomas (functioning) or pNETs may lack the ability to produce hormones (non-functioning), leading to abdominal pain, intra-abdominal bleeding, jaundice, and increased mortality through metastasis.2,3 The likely mechanism of the hematoma in this patient was metastasis to subcutaneous nodules in the lower left abdomen with subsequent hemorrhaging from the vasculature of the metastatic tumor given the presence and location of subcutaneous nodules at the site of the hematoma. Although no biopsy results of the nodules were available, protein tumor markers such as chromogranin A (CgA) and synaptophysin would be expected to be elevated in these neuroendocrine metastatic lesions (our patient had an elevated CgA of 671 ng/mL (ref: 0-187 ng/mL) on arrival).4 While over half of NFpNETs can present with distant metastases, subcutaneous metastases from pNETs are very rare with less than 50 documented cases.4–6
Hemorrhagic metastases have shown a propensity to disperse through vascular invasion, neovascularization, or malignant infiltration as opposed through regional lymph nodes, indicating a potential connection with endothelial or fibroblast growth factors to hemorrhagic metastatic formation to distant cutaneous regions.6,7 The subcutaneous location of the newly discovered nodules also risks bleeding from mechanical stress or mild trauma given the lack of dense tissue support and vessel friability surrounding more superficial areas. Surgical removal of both the primary and distant tumors increases survivability. Our patient had no known personal or family history of coagulopathy or bleeding disorders. Following a provoked deep vein thrombosis (DVT) secondary to immobility after a craniotomy two years prior, she was started on apixaban 5 milligrams twice daily. After the formation of a hematoma, apixaban was discontinued, and the patient underwent placement of an inferior vena cava filter during her hospitalization. Decisions regarding anticoagulation in the context of both a high risk of hypercoagulability (previous DVT and current malignancy) and a high risk of bleeding are critical. This often represents a double-edged sword, as such patients face significant risks of recurrent thromboembolic events due to hypercoagulability and inadequate clot formation in the setting of active hemorrhage. Once the hematoma was managed, the patient was discharged without further anticoagulation therapy through a process of shared decision-making.8
Overall, NFpNETs can metastasize and induce both mass-effect symptoms and in rare instances, sudden hematoma formation. Awareness of this adverse development is essential when monitoring the status of NFpNETs and assessing treatment options such as surgical removal or medical management to stabilize tumor spread/growth and maximize their prognosis.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest
Corresponding author
Farzana Hoque, MD, MRCP, FACP, FRCP
Associate Professor, Department of Medicine
Saint Louis University School of Medicine, St. Louis, MO, USA
Email: farzanahoquemd@gmail.com