
Background
Sarcomatoid cancer of unknown primary site (SCUP) with spine metastasis as its primary presentation is an exceedingly rare clinical entity that poses a uniquely challenging diagnostic and therapeutic prospect. Treatment options for SCUP are scarce and only modestly effective. Prognosis in patients with this disease is poor, with a median overall survival (OS) of around 11 months based on limited published literature. Poor prognostic factors for OS include poor performance status, greater than one metastatic site, elevated lactate dehydrogenase (LDH), and elevated neutrophil-lymphocyte ratio (NLR). Our report describes a case of SCUP with extensive skeletal metastases with rapid clinical deterioration. Early recognition of this disease may aid hospitalists and oncologists to accurately prognosticate, and risk stratify patients with this malignancy.
Case Presentation
A 69-year-old woman presented to the hospital with a chief complaint of low back pain for five months, in addition to three weeks of urinary incontinence. Low back pain was gradually progressive and was associated with radiating, lancinating pain over the posterior aspect of the right lower extremity. She experienced paresthesia and diminished sensations over the right lower extremity, right groin, and right-sided saddle region. She also reported multiple episodes of urinary incontinence and weight loss of about 30 lbs. over the preceding three months. The remainder of her review of systems was unremarkable. Neurological examination revealed weakness and diminished sensation in the right lower extremity in a pattern consistent with CES. Notably, reflexes were normal in all extremities, and rectal tone was preserved. The remainder of the physical exam was unremarkable.
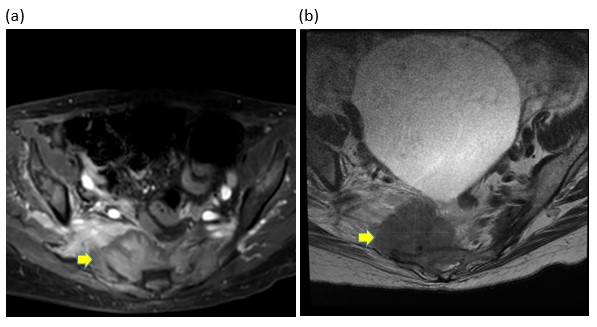
On admission, blood counts and serum chemistries were unremarkable except for mild anemia. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels were elevated at 84 mm/hour and 18.1 mg/dL respectively. Urinalysis and culture ruled out urinary tract infection as a cause for retention and overflow incontinence. Urgent magnetic resonance imaging (MRI) of the whole spine with contrast revealed multifocal areas of marrow replacement in the sacrum and adjacent bilateral iliac bones with a soft tissue mass centered at the right sacral ala infiltrating the right sacral neural foramina (S2-S4) causing cauda equina compression, and marrow replacement of L3, L4, and L5 vertebral bodies (Figure 1). There were additional lesions in the cervical and thoracic spine without spinal cord compression. These multifocal spine lesions were highly suggestive of metastatic cancer. Computed tomography (CT) of the chest, abdomen and pelvis with intravenous contrast revealed multiple bilateral pulmonary metastases. Whole-body Tc-99-MDP scan revealed extensive bony metastases involving the left proximal femur and left distal tibia in addition to the known lesions described.
_centered_around_the_right_sacral_ala_noted_o.jpg)
Needle biopsy of the sacral mass revealed morphology consistent with metastatic sarcomatoid carcinoma with spindle-cell morphology. Immunohistochemistry analysis showed that the tumor cells were positive for CAM 5.2, CK7 and GATA3, with desmin positivity noted mostly in the vascular walls (Figure 2). The immunoprofile was suggestive of urinary bladder or breast origin. Cystoscopy with urine sampling and multiple random bladder wall biopsies was negative for signs of primary cancer. Neither the clinical exam nor CT of the chest was revealing for primary breast cancer.

The patient underwent right total hip arthroplasty for an impending pathological femoral neck fracture. Unfortunately, she had a difficult hospital course after the surgery due to multiple medical complications, including rectal bleeding requiring multiple packed red cell transfusions, and bowel perforation managed conservatively with antibiotics. She began a course of palliative radiation to the lumbosacral region and declined further treatment after the first session. After further discussion with the patient and her family regarding treatment goals, she decided to pursue hospice and comfort care measures. She was discharged to an inpatient hospice facility. She died within a few months after diagnosis due to her widespread cancer.
Discussion
Sarcomatoid carcinomas are aggressive cancers characterized by the presence of both epithelial and sarcoma-like elements. Sarcomatoid transformation has been described in a number of primary epithelial tumor sites, most commonly in cancers of the lung, genitourinary tract, breast and pancreas, among others. A diagnosis of sarcomatoid carcinoma is rendered if greater than 10% of the tumor exhibits sarcomatoid elements. They are believed to arise through divergent differentiation from a single clonal cancer cell.1 The mechanism of its oncogenesis is possibly through epithelial-mesenchymal transition (EMT), a process that is crucial and common during embryological development, but one that remains mostly dormant during adult life. EMT encompasses multiple dynamic processes that involve the loss of epithelial features and the acquisition of mesenchymal properties. These changes include, among others, loss of cell-cell adhesion, decreased expression of cytokeratins and increased expression of mesenchymal proteins like vimentin, smooth muscle actin and fibronectin.2,3
Sarcomatoid carcinomas do not have unique clinical characteristics differentiating them from other cancer histologies at that site. Like most aggressive cancers, they are typically rapidly growing and frequently noted to have metastasized to distant organs at the time of diagnosis. A review of the literature suggests that sarcomatoid carcinoma with spine metastases at presentation is rare, as described in a case report by Arshad et al.4 The case described an instance of metastatic spindle-cell sarcomatoid carcinoma to the thoracic spine arising from a lung primary site in a 63-year-old patient with HIV infection. After undergoing resection of the thoracic tumor, he was treated with a combination chemotherapy regimen consisting of gemcitabine and paclitaxel.
Diagnostic workup of SCUP, like all cancers of unknown primary site (CUP) regardless of histology, begins with a computed tomography (CT) scan of the chest, abdomen and pelvis with intravenous (IV) contrast. Workup should include breast imaging for women and prostate-specific antigen (PSA) measurement in men. Additionally, site-directed evaluations can be performed in cases where there are other laboratory abnormalities (for instance, diagnostic colonoscopy in patients with blood loss anemia).5 The role of PET-CT in the evaluation of CUP is unclear. Some studies suggest that PET-CT is not superior to CT alone in the detection of the site of origin.6 The advent of sophisticated tumor profiling by immunohistochemistry and tissue-of-origin molecular profiling assays has greatly improved the identification of primary sites in patients with SCUP. IHC testing is reliant on the principle that both the primary tumor and its metastatic sites share a similar protein expression profile.7 In our patient, IHC studies posited that the site of origin was likely to be the urinary bladder or breast, but further site-directed evaluation of these sites did not yield evidence of the primary cancer.
Microscopic examination with immunohistochemical studies of biopsy tissue is the gold standard of diagnosis for SCUP. On light microscopy, the characteristic finding in these cancers is the presence of mixed epithelial and mesenchymal elements. Desmin and vimentin are the most common mesenchymal markers. Pankeratin markers (AE1/AE3, CAM 5.2) are positive in most carcinomas. Tumors with a significant spindle-cell component, particularly those arising from the lung, stain positively for cytokeratin 7 (CK7) in about 70% and thyroid-transcription factor-1 (TTF-1) in about 55% of cases.8 Our patient’s tumor biopsy sample stained positive for CAM 5.2, CK7 and GATA3 (which is typically seen in cancers of the lower urinary tract).
There is a steadily increasing prominence of specialty neurosurgical co-management hospitalist services at academic centers in the United States.9 With that in mind, it becomes imperative for hospitalists to expeditiously recognize and manage patients with CES on the hospital floors. Regardless of etiology, CES is a neurosurgical emergency, and expedient treatment is essential to achieve functional neurological recovery. Urgent neurosurgical consultation and evaluation for decompressive surgery is a critical first step in the management of CES. The presence of urinary incontinence and extensive perianal anesthesia at presentation portend poor postoperative functional recovery. Surgical decompression of the cauda equina within the first 48 hours after initial presentation is associated with improved neurological recovery.10 In cases of CES from metastatic cancer such as in this instance, hospitalists can liaise effectively with surgical, oncological, and palliative care teams to oversee personalized and patient-centered treatment plans.
There is currently a lack of evidence-based clinical treatment guidelines for the management of sarcomatoid cancers of any primary site. To date, there have been no prospective randomized clinical trials to inform treatment guidelines for this disease. Typically, expert consensus recommendations have been to treat sarcomatoid cancers with surgery, if resectable, and standard site-specific chemotherapy and/or radiation regimens.11,12 SCUP poses an added layer of complexity to treatment due to the occult nature of the primary cancer, and chemotherapy resistance is not uncommon in these cases. A retrospective review of 48 metastatic sarcomatoid cancers from the MD Anderson database showed that chemotherapy was the most frequently utilized first-line treatment (35% of cases). The most common agents used were gemcitabine and docetaxel, as this pairing has shown activity against a wide variety of carcinomas and some sarcomas. Unfortunately, most cancers (77% of cases) progressed within 2 months despite chemotherapy.13 Palliative radiation is a useful adjunct for symptom relief, particularly in cases of spinal cord compression and significant cancer-related pain from skeletal metastases.14
Cancer treatment has undergone a paradigm shift over the last few decades with the advent of newer targeted therapies and immunotherapy agents. The treatment landscape of sarcomatoid cancer of any primary site has been relatively immune to this change due to its rarity and relatively unknown tumor biology. However, several small studies over the past decade have attempted to characterize genomic alterations in SCUP via whole-exome sequencing. In sarcomatoid cancers of the lung and kidney, PD-1 and PD-L1 expression was found to be significantly higher than in non-sarcomatoid phenotypes of RCC, which potentially suggests a role of immune checkpoint inhibitors in selected patients.15 There have also been studies involving pulmonary sarcomatoid cancers (PSCs) showing the presence of potentially targetable genomic alterations.16,17 Another study analyzing 36 cases of PSCs using whole-exome sequencing identified targetable MET exon 14 skipping alterations in 22% of tumors, suggesting a promising role for tyrosine kinase inhibitors (TKIs; e.g. savolitinib, capmatinib, and crizotinib) that have proven activity against this alteration.18The treatment landscape for SCUP currently is limited, although it is rapidly evolving. Despite the paucity of randomized clinical trials to guide treatment decisions, an ever-expanding understanding of tumor biology through studies utilizing next-generation sequencing (NGS) techniques may offer some patients with SCUP effective treatment options.
Acknowledgments
Publication made possible in part by support from the Thomas Jefferson University Open Access Fund.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest
Corresponding author
Bharath Ganesh M.D.
Assistant Professor of Medicine
Farber Hospitalist Division of Neurological Surgery
Departments of Medicine and Neurological Surgery
Thomas Jefferson University
909 Walnut Street, suite 320
Philadelphia PA 19102
E-mail: bharath.ganesh@jefferson.edu
Phone: (215)955-7000