Background
A Meckel’s diverticulum occurs when there is incomplete atrophy of the vitelline (omphalomesenteric) duct during early development at 5-7 weeks. This ectopic gastric tissue predisposes patients to hyperacidity due to excessive acid-producing oxyntic cells and resultant mucosal ulceration leading to GI bleeding.1 This accounts for the characteristically painless bloody stool seen when symptomatic patients present with a Meckel’s diverticulum. We present a patient with abdominal pain and vomiting who was found to have intussusception and perforated Meckel’s diverticulum.
Case Presentation
A 2-year-old previously healthy male presented to the emergency department (ED) with abdominal pain, non-bloody, non-bilious emesis, and diarrhea. Initial symptoms of emesis began 5 days prior. On the second day of symptoms, patient was taken to an urgent care, diagnosed with acute gastritis and discharged with Zofran. Initially, emesis was controlled but it returned 2 days later. He began experiencing intermittent abdominal discomfort with non-bloody diarrhea and went to his pediatrician. During these periods of pain, the patient would curl up in a ball and cry while refusing to walk or void. Episodes would wax and wane throughout the day, lasting a few minutes without any recognized trigger. An abdominal X-ray ordered by the pediatrician showed a nonspecific abdominal bowel gas pattern with scattered stool and air throughout the colon. No signs of obstruction were identified. He remained afebrile and had no known sick contacts, travel, or daycare exposure. The patient was referred to the ED.
In the ED, the patient cried with abdominal exam but tolerated gentle palpation with some guarding. An initial ultrasound looking for appendicitis and intussusception demonstrated right lower quadrant bowel wall edema, and hazy free fluid but no other acute changes. An abdominal computed tomography (CT) scan with intravenous and oral contrast showed no appendicitis or other pathology. There was mildly increased wall thickness of the distal small bowel loops thought to represent peristalsis versus enteritis. Right abdominal small bowel loops appeared mildly distended with air-fluid levels suggesting ileus. A comprehensive metabolic panel, complete blood count, and lipase were within normal limits (Table 1). A urinalysis showed small ketones consistent with dehydration. Patient received fluids and was discharged.
The patient remained at home for approximately 8 hours before returning to the ED with episodic abdominal pain. These episodes were occurring at least twice per hour for 3-5 minutes at a time, and were associated with abdominal guarding, crying, and inability to tolerate oral intake. He had loose, non-bloody stools, but an extensive GI infection array testing was negative. The surgical team recommended observation. Repeat abdominal ultrasound showed multiple peristalsing bowel loops and a small amount of trace ascites in the bilateral lower quadrants, but was otherwise negative. Patient was admitted for rehydration and observation.
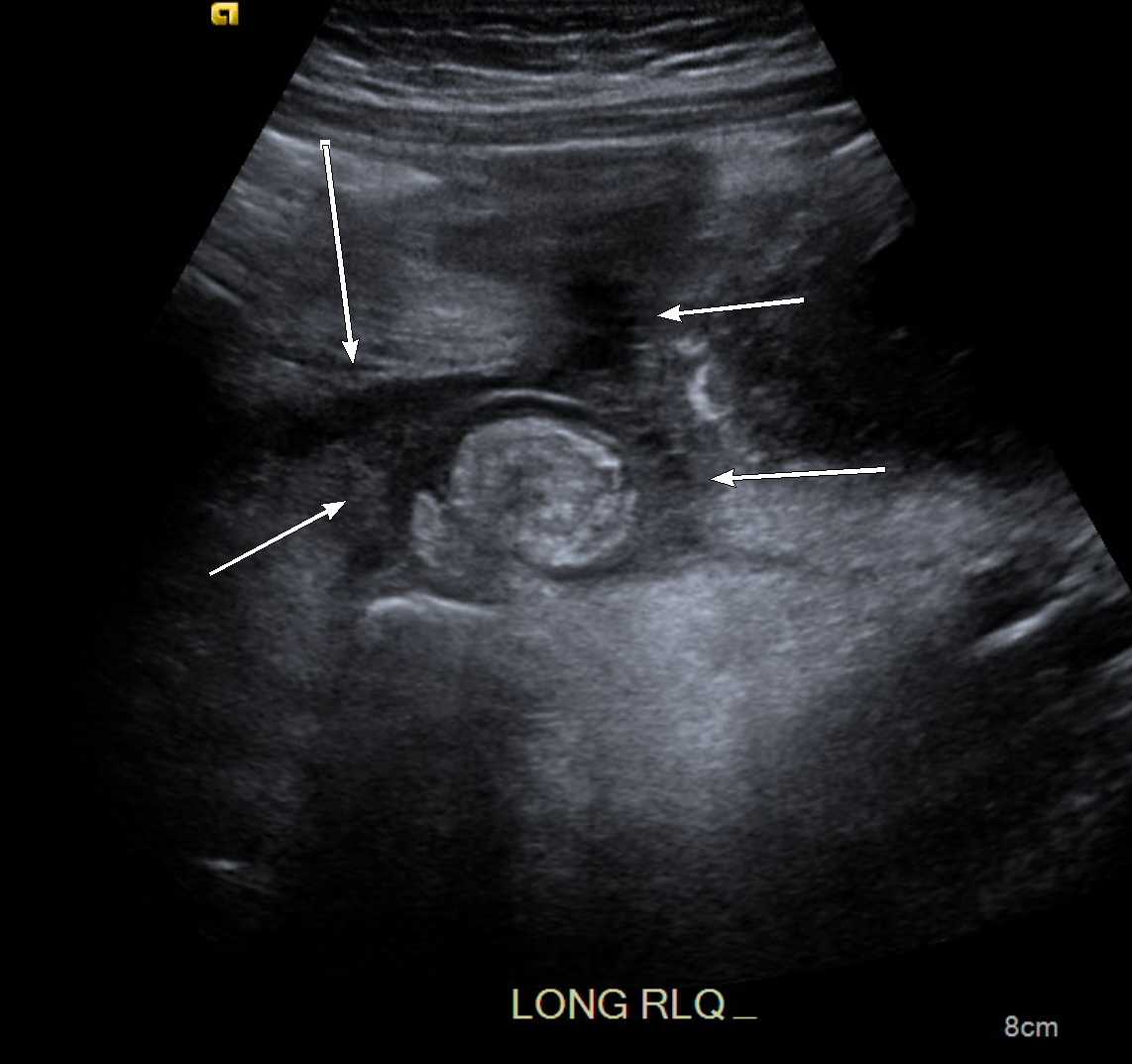
Later that day, the patient developed reddish–brown stool that was fecal occult positive. The patient’s abdomen became distended with diffuse tenderness to palpation; he was described as fussy and fought examination during an acute episode of pain. A stat ultrasound was obtained during an acute episode of pain showing a classic “target sign” ileo-ileal intussusception that persisted throughout imaging with thickened distal small bowel loops and hazy free fluid (Figure 1). These findings were attributed to an enteritis versus an occult Meckel’s diverticulum. Given the patient’s progression and pain, surgery was reconsulted and took the patient emergently to the operating room. A diagnostic laparoscopy was converted to an open laparotomy due to significant adhesions and inflammation. There was no longer a persistent intussusception identified but surgical inspection revealed a perforated Meckel’s diverticulum. The perforated area of the small bowel was resected, and patient had an uneventful postoperative course and recovery.

Surgical pathology confirmed the diagnosis as acute Meckel’s diverticulitis with acute serositis. Microscopic examination showed portions of a Meckel’s diverticulum lined by small intestinal mucosa with areas of ulceration and acute inflammation. A focal perforation was present with associated serosal edema, acute fibrinopurulent serositis, and fibrinous adhesions.
Discussion
This patient had a Meckel’s diverticulum that served as a lead point for intussusception and diverticulitis with perforation. Complications of Meckel’s diverticulum are rare in children. Of the approximate 2% of the population who have a Meckel’s diverticulum, complications occur in only about 4%.2 If symptoms develop in children, it is usually painless bloody stool, but up to 22–50% of children/adults can present with signs of intestinal obstruction. In these cases, the Meckel’s diverticulum can serve as a lead point for the intussusception and has been noted to occur in roughly 14% of cases in children.3,4 Other mechanisms by which a Meckel’s diverticulum can cause obstruction include a volvulus, impacted meconium, and enteroliths to name few.3
Given the intermittent nature of abdominal pain, there was a high initial suspicion for intussusception in this patient. Studies have shown that the triad of intermittent abdominal pain, vomiting, and a right upper quadrant abdominal mass can have a positive predictive value as high as 93% for intussusception.5 This patient had two out of those three symptoms although no mass had ever been palpated. It was not until the third abdominal ultrasound was obtained that an ileo-ileal intussusception persisted throughout imaging. Generally speaking, ultrasounds have a sensitivity of 98.5% and specificity of 100% for diagnosing intussusceptions. While barium enemas may be the gold standard of diagnosis, generally an ultrasound is sufficient to diagnose a simple intussusception and has few false negatives.6 Ideally, ultrasounds should be obtained during an acute episode of pain to successfully diagnosis intussusception; for this patient he was diagnosed only when the ultrasound was obtained during a painful paroxysm.
In terms of a Meckel’s diverticulum serving as the lead point of the intussusception, it is important to note that CT and ultrasounds are unable to distinguish between a Meckel’s diverticulum verses a loop of bowel. In cases where there is a high suspicion of a Meckel’s diverticulum, a 99mTc- pertechnetate scan should be obtained and remains the gold standard for diagnosis of Meckel’s.7 Given the low prevalence, there are no standard of care recommendations for performing a Meckel’s scan when intussusception is suspected, though it should be kept in the differential diagnoses.
For this particular patient, given his worsening abdominal exam and worsening pain, in conjunction with an ileo-ileal intussusception on ultrasound, he was taken to surgery where the diagnosis of a perforated Meckel’s diverticulum was made. Interestingly, treatment for intussusception varies based upon location of the intussusception. If it is ileocolic, the most common location, it is reachable and reducible with an air enema. When it is located within the small bowel or ileo-ileal, usually they reduce spontaneously. If not, usually surgery is needed because the air enema is ineffective at reaching and reducing the troubled part of the bowel.8
Additionally, this patient had a perforation. Due to the nature of ectopic gastric tissue, a Meckel’s diverticulum can cause bowel necrosis, sepsis, and perforation from progressive inflammation or ulcerating ectopic tissue.7,9 However, all of these complications are rare and diverticulitis with perforation has been estimated to occur in only 12% of children.4 For this reason, treatment of a symptomatic or complicated Meckel’s diverticulum involves surgical resection to remove the ectopic gastric tissue. Resection of a symptomatic Meckel’s diverticulum eliminates increased risk of persistent bleeding.1 This was performed in our patient so that he could recover completely with no longstanding side effects from the symptomatic Meckel’s diverticulum.
This case highlights the importance of maintaining a broad differential when patients present with symptoms consistent with common diagnoses, such as gastroenteritis, which can lead to anchoring biases. This patient had no fever or evidence of infection and, coupled with worsening pain, this prompted further investigation. Ultimately this led to the diagnosis of a perforated Meckel’s diverticulum which initially masqueraded as an intussusception. In this particular case, an ultrasound taken during an acute episode pain was crucial to making a diagnosis and taking the next steps towards treatment.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest
Corresponding Author
Sarah Marzec, MD, MA
700 Children’s Drive, FB3164,
Columbus, OH 43205
Phone: 614–722-5230
Fax: 614-722-5115
Email: sarah.marzec@nationwidechildrens.org