Background
Cardiac involvement by lymphoma is a rare and underdiagnosed, but increasingly recognized occurrence. Recent estimates of its incidence range from 8.7% to 20% as identified by autopsy.1 Cardiac involvement can be primary (also called primary cardiac lymphoma), involving only the heart and/or pericardium, or secondary to disseminated lymphoma. Secondary disease is significantly more common, as primary cardiac lymphoma accounts for less than 2% of cardiac tumors, and less than 1% of extranodal lymphomas.2–4
Case Presentation
A 66-year-old male with a past medical history of hypertension and non-obstructive coronary artery disease presented to the Emergency Department with chest heaviness. Three months prior to his presentation, he began to experience constant, non-exertional chest pain and discomfort that was associated with significant dyspnea. He also endorsed night sweats, hot flashes, early satiety, and unintentional weight loss over this period. His symptoms continued, and one month prior to presentation, he also noted fullness around his neck on both sides, which prompted him to present to an outside hospital. There, a CT neck and chest was performed, which was notable for a “large 3.7 cm right atrial filling defect suspicious for thrombus versus neoplasm” and extensive bilateral cervical, intrathoracic, and upper retroperitoneal lymphadenopathy suspicious for nodal metastases versus lymphoma. Based on these findings, he was recommended to present to our institution for expedited evaluation and treatment. History was also notable for an extensive family history of cancer: hepatocellular carcinoma in his father, breast cancer in his mother, lung cancer in his maternal grandmother, and prostate cancer in his maternal uncle. Home medications that the patient was taking were amlodipine 5 mg daily, aspirin 81 mg daily, and atorvastatin 40 mg daily.
On admission, the patient was hemodynamically stable without vital sign abnormalities. Physical exam was notable for multiple firm, enlarged, and non-tender cervical and supraclavicular lymph nodes, with the largest nodes palpable in the right supraclavicular area. The remainder of his physical exam, including neurologic, cardiopulmonary, and skin exams, was normal. Laboratory testing demonstrated a mild normocytic anemia (hemoglobin 13.1 g/dL (normal: 13.5-17.1 g/dL) with mean corpuscular volume 91.4 fL (normal: 79.3-98.6 fL)) and a high-sensitivity troponin of 13 ng/L (normal: < 5 ng/L) which remained stable on subsequent measurement. The remainder of his admission labs, including chemistry panel, liver enzymes, coagulation studies, and iron panel, were within normal limits. Brain natriuretic peptide (BNP) was normal at 85 pg/mL (normal: < 100 pg/mL), and HIV 1/2 Ag/Ab screen was negative. His electrocardiogram (ECG) showed normal sinus rhythm with a rate of 73, prolonged PR interval of 220 msec, and left atrial enlargement. Chest X-ray revealed borderline cardiomegaly and a prominent upper mediastinum.
A transthoracic echocardiogram was performed, demonstrating normal left ventricular systolic function at 65-70%, a small circumferential pericardial effusion without any evidence of tamponade, and a mildly enlarged aortic root (4.1 cm) and mid-ascending aorta (4.0 cm). The right atrium was poorly visualized, with a potential view of the mass vs. artifact noted on a singular clip. The patient’s prior outside CT scans were interpreted at our facility with similar findings: extensive bilateral lower cervical, mediastinal, hilar, and axillary lymphadenopathy causing moderate-severe narrowing of the left upper lobar pulmonary artery branch and left upper and lower lobar bronchi, in addition to mild narrowing of the inferior superior vena cava (SVC) at the cavoatrial junction. The intra-atrial mass versus filling defect in the right atrium was measured at 3.7 x 3.7 cm. These findings were overall concerning for a lymphoproliferative disorder or metastatic intrathoracic disease. Given the presence of multiple superficial enlarged lymph nodes, Interventional Radiology was consulted and performed an ultrasound-guided biopsy of a left supraclavicular lymph node.
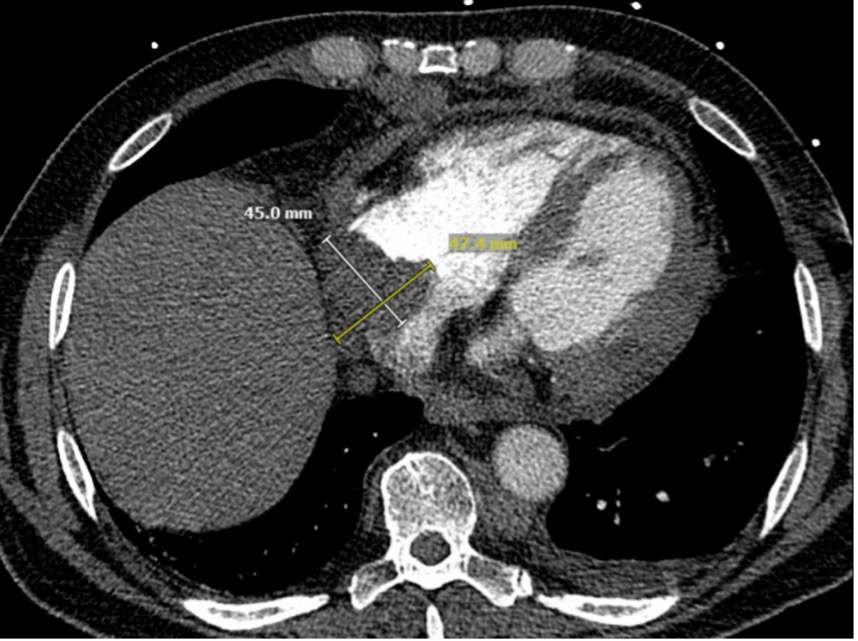
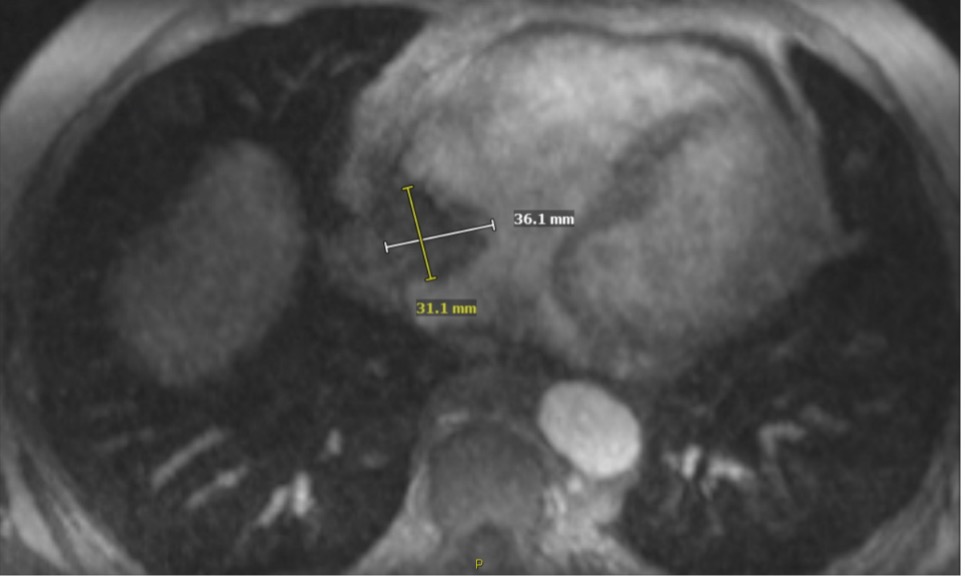
While awaiting pathology results, additional imaging was pursued. CT chest angiogram noted a right atrial mass suspicious for lymphoma as the cause of the right atrial filling defect (Figure 1a). Next, a cardiac MRI was performed, showing the lobulated right atrial mass infiltrating into the chamber wall and extending into the pericardial space, with pericardial thickening and a small pericardial effusion (Figure 1b). Lastly, for staging purposes, a CT abdomen pelvis was performed, demonstrating enlarged periportal, retroperitoneal, retrocaval and iliac and inguinal lymph nodes along with mild splenomegaly. After several days, the lymph node biopsy resulted with diffuse large B-cell lymphoma, germinal-center type, elucidating a unifying diagnosis for his lymphadenopathy and cardiac mass, which was felt to be a secondary cardiac lymphoma given his widespread lymphadenopathy. His peripheral smear showed lymphopenia but no evidence of abnormal cells, and his peripheral flow cytometry was within normal limits.


The patient’s hospital course was complicated by an episode of sustained tachycardia triggered by exertion. He experienced sudden-onset palpitations upon standing, with an acute increase in heart rate from 80 to 135 beats per minutes with a narrow QRS complex. His blood pressure remained normal throughout this episode. Vagal maneuvers were attempted without resolution of tachycardia. ECG revealed supraventricular tachycardia at a rate of 130 beats per minute with potential 2:1 atrioventricular block. Adenosine 6 mg IV was given, revealing atrial flutter as the underlying rhythm. He was then given metoprolol tartrate 5 mg IV and magnesium repletion, with successful conversion to sinus rhythm. He was also started on metoprolol tartrate 25 mg twice daily. Complete blood count (CBC), chemistry panel, thyroid function tests, and cardiac biomarkers were rechecked and within normal limits, revealing his atrial mass to be the likely trigger of this episode. Given his ongoing risk of paroxysmal atrial arrhythmia, he was started on a heparin drip at therapeutic dosing and transitioned to apixaban prior to discharge. He was subsequently discharged with plan for outpatient oncologic treatment and serial cardiac imaging to monitor the cardiac mass.
Two weeks after discharge, he began induction therapy with dose-adjusted R-EPOCH (rituximab, etoposide phosphate, prednisone, vincristine sulfate, cyclophosphamide, and doxorubicin hydrochloride), with each cycle of chemotherapy being completed in the inpatient setting given his high risk of complications. The first cycle was complicated by atrial fibrillation and flutter with rapid ventricular response requiring an amiodarone load and increase in his metoprolol dosing. He was also found to have enlargement of his pericardial effusion on CT imaging, as well as pericardial thickening and small-to-moderate pleural effusions concerning for both pericardial and pleural lymphomatosis. Serial repeat transthoracic echocardiograms were negative for further enlargement or any evidence of tamponade. Cycles two through four were administered without complications. Repeat cardiac MRI after two cycles of treatment demonstrated an interval decrease in the size of the right atrial mass, measuring 2.1 cm. Interval PET-CT after cycle three demonstrated resolution of the cardiac mass and resolved lymphadenopathy aside from an isolated lesion in the right iliac chain. Unfortunately, repeat PET-CT after cycle four demonstrated progression in size of the iliac node, indicating disease refractory to first-line therapy. He is now approximately 5 months from diagnosis, and second-line therapy is currently being determined.
Discussion
Cardiac lymphomas most often arise in the pericardium or the right heart, particularly in the right atrium, in both primary and secondary cases.2,3,5 They are most commonly due to diffuse large B-cell lymphoma, followed by Burkitt lymphoma, T cell lymphoma, small cell lymphoma, and plasmablastic lymphoma.2,4,6 Cardiac involvement is generally a late manifestation of disseminated disease and is frequently undetected before death due to lack of specificity of clinical symptoms and difficulty in obtaining pathologic samples. Clinical presentation is variable, and can be asymptomatic or present with nonspecific cardiac signs and symptoms including heart failure syndromes, chest pain, arrhythmias, or constitutional symptoms.
Transthoracic echocardiography is thus the screening modality of choice, though is known to be limited and less sensitive than transesophageal echocardiography; while nonspecific, pericardial effusion is found in the vast majority of patients at presentation.1,4,6 CT imaging is advantageous for showing morphology, location, and extent of tumor burden, while PET-CT can reveal previously unsuspected cardiac involvement. Cardiac MRI, on the other hand, best identifies anatomy, blood flow, and extent of myocardial and pericardial involvement. There are no definitive treatment guidelines specific for lymphoma with cardiac involvement, but it is generally managed with systemic chemotherapy and periodic imaging tailored to each individual patient. Unfortunately, the presence of a cardiac mass in lymphoma indicates an aggressive form of disease and confers a poorer prognosis.6,7
Our case demonstrates several considerations in effectively diagnosing and treating lymphoma with cardiac involvement. First, that transthoracic echocardiography is a limited modality when evaluating for cardiac masses. Although our patient had a known right atrial thrombus or mass based on prior CT imaging, his initial TTE poorly visualized the right atrium, with only one potential view of the mass despite its relatively large size. It is important, therefore, to proceed with transesophageal echocardiography (TEE), CT, or cardiac MRI before ruling out the presence of a cardiac mass. Next, this case demonstrates the effectiveness of a minimally invasive approach to tissue biopsy for establishing diagnosis. Traditionally, tissue biopsy of cardiac masses required thoracotomy.1,7 However, multiple less invasive methods of tissue sampling now exist, including diagnostic lymph node biopsy, pericardial fluid cytology sampling, TEE-guided cardiac biopsy, endomyocardial biopsy, and percutaneous intracardiac biopsy, depending on the patient presentation. Given that our patient presented with extensive lymphadenopathy in both superficial and deep compartments, we were able to proceed with a simple percutaneous ultrasound-guided biopsy of a single supraclavicular lymph node under local anesthesia. In doing so, we avoided the risks of more invasive tissue sampling procedures and more substantial anesthesia while also gathering the specimen necessary to efficiently establish his diagnosis.
Finally, our case highlights the potential life-threatening complications of arrhythmia and pericardial effusion in the natural history and treatment of cardiac lymphomas. Although arrhythmias are a known potential presenting symptom and complication of cardiac masses, specific instances have been infrequently documented. Given that our patient’s cardiac mass was in the right atrium, direct mass effect and atrial stretching likely predisposed to the development of atrial flutter with rapid ventricular response. This arrhythmia recurred after his first cycle of chemotherapy despite rate control, potentially triggered by the rapid cytoreduction that often occurs with induction therapy in rapidly proliferating hematologic malignancies. While infrequent, other potential fatal complications specific to cardiac masses in the early post-chemotherapeutic period include ventricular fibrillation, refractory heart failure, and even cardiac rupture from rapid tumor destruction.1,6 Fortunately, the arrhythmia encountered by our patient during the post-chemotherapeutic period was transient, did not lead to hemodynamic instability, and responded to first-line rate and rhythm control agents without degeneration into a malignant arrhythmia. In summary, cardiac lymphomas are more common than previously recognized, and must be effectively evaluated, diagnosed, and treated in order to improve patient outcomes.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest
Corresponding Author
Ramzy Jandali MD,
UCLA Ronald Reagan Medical Center,
Department of Medicine – Los Angeles, CA, USA
Email: rjandali@mednet.ucla.edu
Phone: 818-337-9093