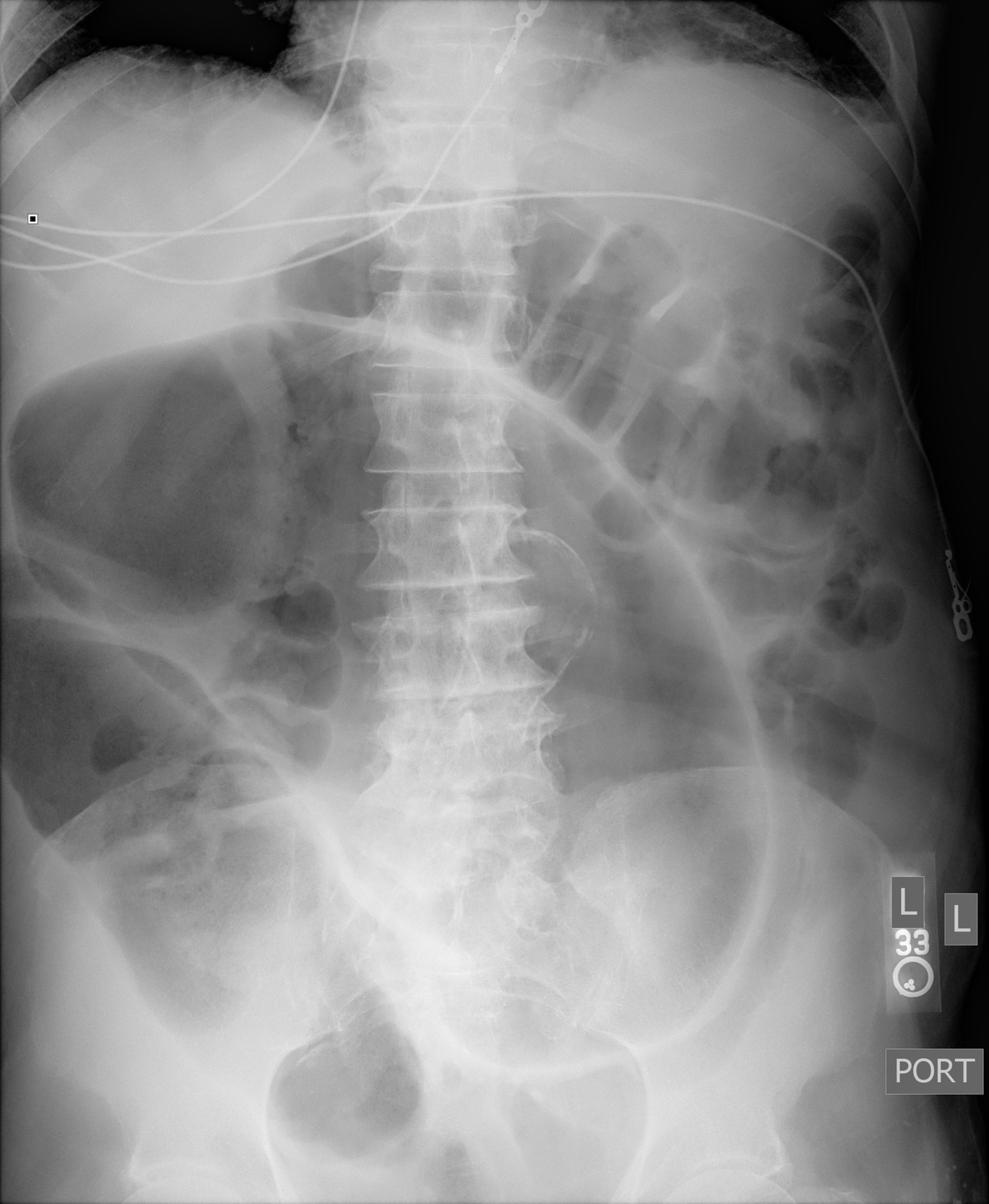

A 99-year-old man presented to the hospital with four days of progressive abdominal pain and distention accompanied by anorexia and obstipation. Examination revealed a markedly distended, tympanitic abdomen with hypoactive bowel sounds and diffuse tenderness. An abdominal radiograph showed markedly dilated loops of large bowel shaped like a coffee bean (Figure 1). Computed tomography (CT) of the abdomen and pelvis confirmed a severe dilation of the sigmoid colon with twisting of the sigmoid mesocolon and vessels consistent with sigmoid volvulus (Figure 2). The patient underwent flexible sigmoidoscopy for endoscopic decompression and ultimately required colectomy for recurrent sigmoid volvulus.
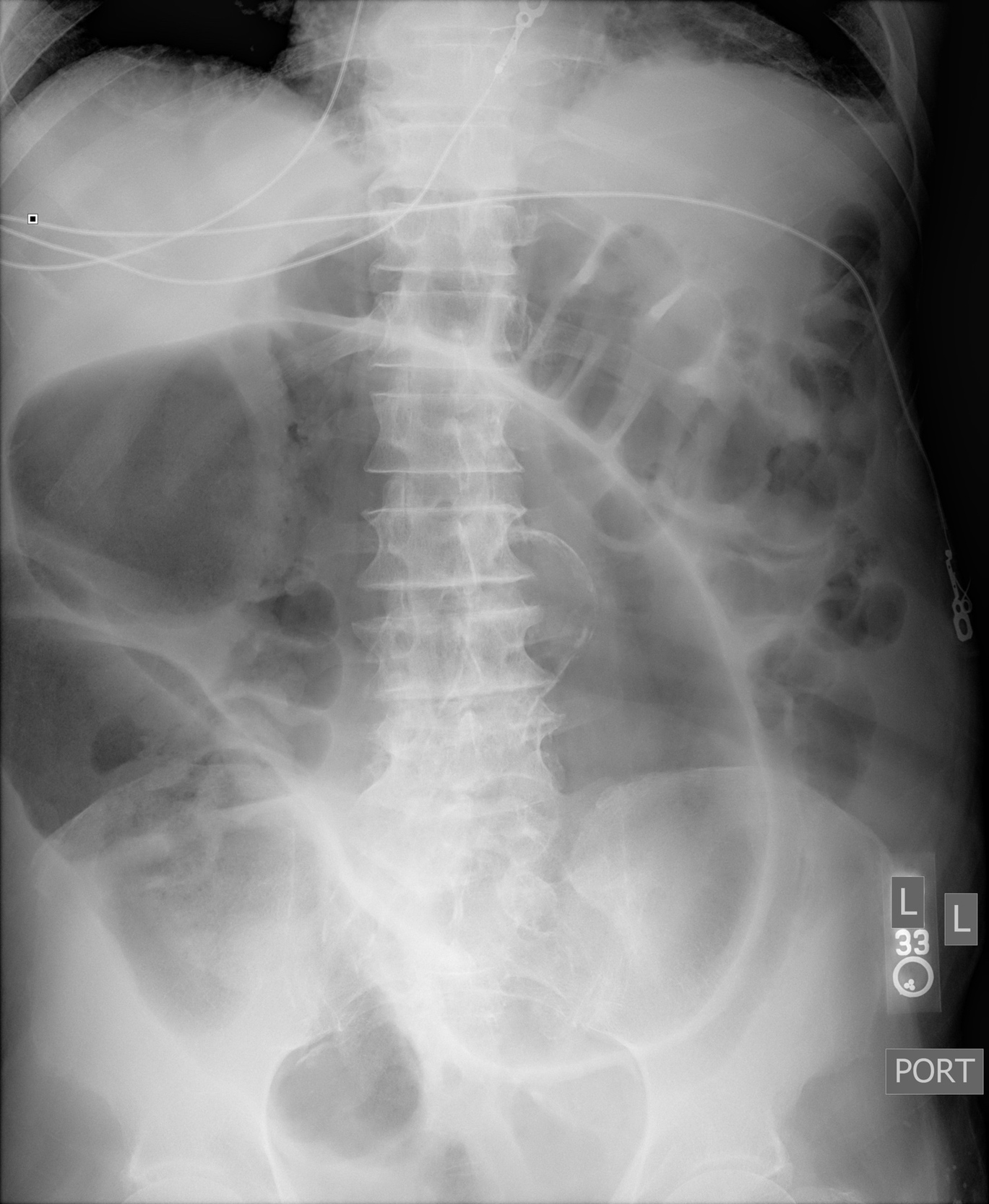

The “coffee bean sign” is a conventional radiographic finding classically associated with the closed loop bowel obstruction in sigmoid volvulus. In sigmoid volvulus there are often multiple dilated loops of large bowel present as adjacent air-filled densities with an inner wall created by two layers of bowel wall abutting one another.1 Often caused by anatomic variations and redundant sigmoid colon, patients at particular risk for sigmoid volvulus include older male patients, nursing home residents, and those with chronic constipation, neurologic disease, and prior abdominal surgery.2 As sigmoid volvulus may quickly lead to bowel infarction and necrosis, timely recognition and distinguishing from mimics such as acute colonic pseudo-obstruction (ACPO) is essential.
While plain radiographs readily detect sigmoid volvulus, CT confirms the diagnosis in most cases through identifying mesenteric twisting.2 Colonic dilation without twisting or a mechanical obstruction suggests a diagnosis of ACPO. Cecal volvulus may present similarly on abdominal radiography but typically demonstrates only a single air-fluid level, in contrast to the two air-fluid levels often seen in sigmoid volvulus.1 CT imaging is likewise necessary for distinguishing between cecal and sigmoid volvulus. Clinicians should carefully review the radiograph and CT images for pneumatosis intestinalis, which suggests arterial ischemia, and pneumoperitoneum, which indicates bowel perforation, both of which constitute surgical emergencies.2
The management of sigmoid volvulus includes urgent endoscopic decompression via flexible sigmoidoscopy which confirms the diagnosis, assesses the viability of the bowel, and bridges to definitive surgical management with colectomy. While endoscopic detorsion is effective at reversing volvulus, elective colectomy should be performed within two to five days given the high incidence of recurrent volvulus (40-70%).2
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest
Corresponding Author
Tyler Larsen, MD
11301 Wilshire Blvd
Building 500, Suite 3214-B
Los Angeles, CA 90073
Email: tlarsen@mednet.ucla.edu
Phone: 310-478-3711 x47031