Background
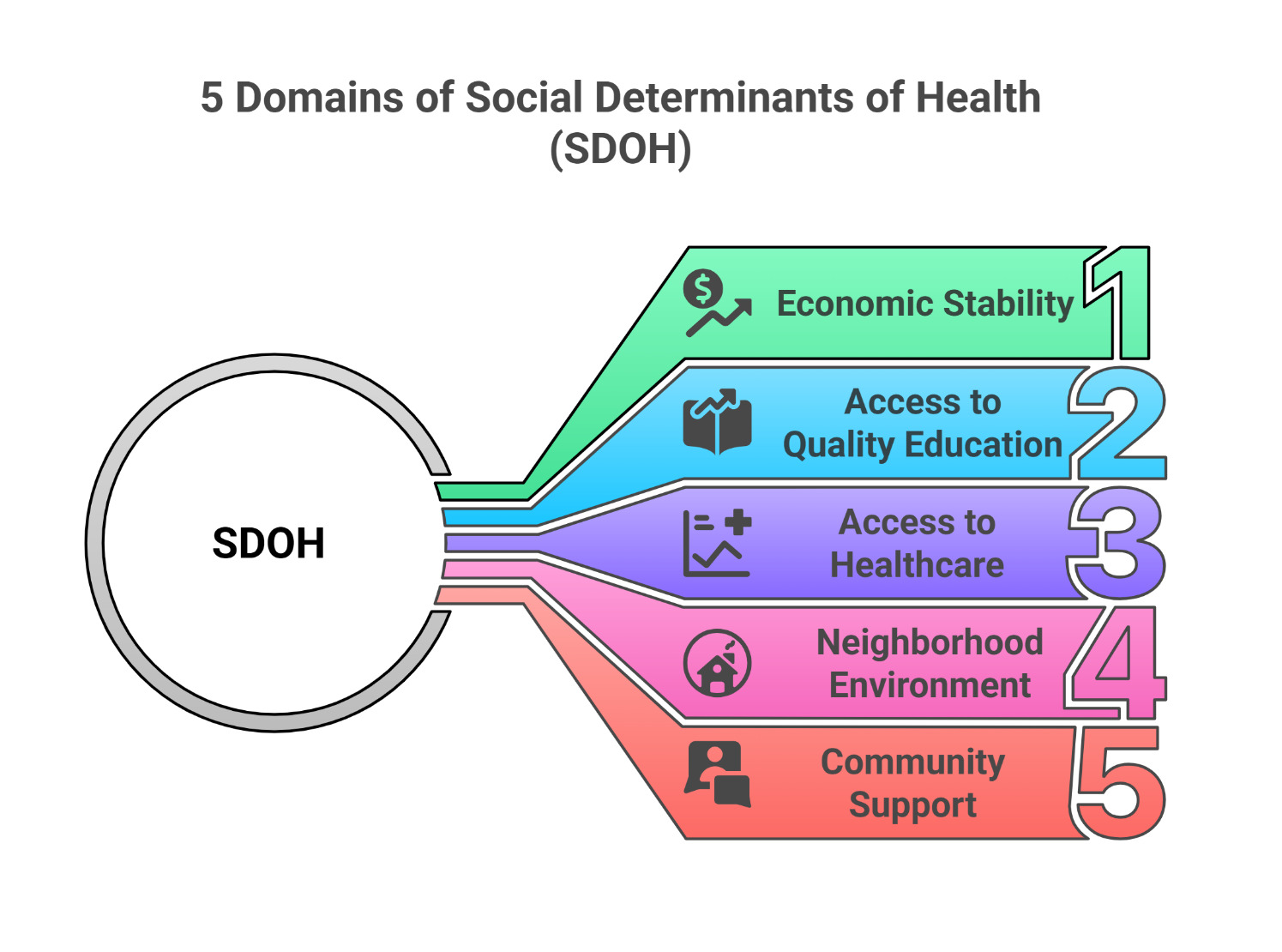
Social barriers are increasingly recognized as contributors to disparities in patient care. These social barriers, often referred to as social determinants of health (SDOH), are the conditions in which people grow, live, learn, and work. SDOH can be grouped into five broad categories: economic stability, access to quality education, quality healthcare, neighborhood environment, and community support (Figure 1). These categories influence health, well-being, and overall quality of life.1,2
Structural factors such as government policies, economic inequality, and neighborhood disinvestment shape patients’ personal challenges when seeking care. These broader conditions contribute to obstacles such as limited transportation options, reduced access to high-quality healthcare, and lower levels of trust in medical providers. By shaping the environments in which people live, learn, and work, these structural determinants lead to individual-level health disparities and poorer outcomes for vulnerable populations.2–4 This review examines how social determinants of health (SDOH) shape a patient’s journey, including the time taken to reach the hospital, the quality of care received, and the discharge process, to highlight their impact on patient healthcare outcomes.
.png)
SDOH Impact on the Journey to the Hospital
Social determinants of health (SDOH) significantly influence patients’ willingness and ability to seek medical care. Low-income individuals frequently encounter challenges such as finding healthcare facilities that accept their insurance and reporting both systemic barriers (e.g., a scarcity of clinics accepting government-assisted insurance) and interpersonal discrimination based on race and socioeconomic status.2,3 Such negative experiences reduce patient-provider trust, discouraging patients from seeking future care.4,5 Limited economic stability further restricts healthcare access through fewer healthcare options and negative stereotyping, perpetuating a cycle that reinforces health disparities. Transportation is another critical SDOH affecting healthcare access. Common issues such as transportation costs, lack of personal vehicles, and long travel distances lead to delayed care and missed appointments, especially among low-income individuals, elderly populations, and those with chronic conditions.6 Difficulties securing transportation or affording alternatives like bus passes hinder timely medical care.7 Missed appointments due to transportation barriers can lead to poor chronic condition management and undiagnosed health problems. Interventions like Medicaid transportation assistance have improved appointment adherence, underscoring transportation’s direct influence on patient outcomes.8Increasing healthcare staff awareness of available transportation assistance programs may further reduce missed appointments and improve outcomes.
SDOH Impact on Patient Care
The patients on Medicaid experience higher rates of adverse safety events, respiratory failure, and sepsis compared to privately insured patients within the same facilities.9 This disparity may result from limited specialized care access and increased comorbidities. Similar disparities exist among low socioeconomic status (SES), Medicaid-insured, and uninsured colon cancer patients, who often receive inadequate lymph node removal and fewer adjuvant chemotherapy treatments, primarily due to their concentration in lower-performing hospitals.10 Additionally, African American patients frequently receive lower-quality care even in high-performing hospitals, indicating persistent barriers such as transportation and insurance gaps.10 Disparities also extend to orthopedic conditions; publicly insured patients commonly experience delays between anterior cruciate ligament (ACL) injury diagnosis, surgery, and post-operative care, leading to poorer recovery outcomes, including reduced strength and limited mobility.11 Thus, insurance type and socioeconomic status significantly influence treatment quality and hospital length of stay.
Clinicians typically spend less time, provide fewer explanations, and build less rapport with low SES patients than higher SES patients.12 Compounded by limited patient engagement, possibly due to perceived discrimination, financial strain, or family responsibilities, these interactions negatively influence patient satisfaction and care perception.13,14 Patients with low SES often report feeling unfairly treated, which adversely affects satisfaction, trust, and overall care outcomes.14 SDOH also influences hospital length of stay. Patients facing housing instability remain hospitalized longer than those with stable housing (6.7 vs. 4.8 days).15 High SES patients typically experience shorter hospital stays due to more stable housing and better access to follow-up care.16 However, shorter hospital stays observed among low SES heart failure patients might reflect limited self-advocacy, as these patients may not actively request services or support.17 Limited outpatient care access further contributes to higher emergency department visits and frequent re-hospitalizations among low SES patients.18 Thus, the impact of SDOH on hospital length of stay varies significantly based on individual circumstances, available resources, and specific health needs.
SDOH Impact on Post-Hospitalization Care
SDOH also critically influences post-discharge recovery. Patients are typically expected to manage new diagnoses, adhere to care routines, and attend follow-up appointments. However, SDOH-related barriers—such as unstable housing, limited resources, and weak social support—complicate these tasks. Patients from disadvantaged neighborhoods are more likely to face repeated hospital re-observations due to limited access to skilled nursing facilities (SNFs).19 The financial burden from repeated re-observation stays is significant, with average costs reaching $528 per stay without a Medicare out-of-pocket cap.20 Programs such as Medicare’s Transitional Care Management (TCM) aim to improve outpatient coordination and reduce preventable readmissions. Although TCM has modestly decreased hospital readmissions, particularly in smaller, independent practices, it has not significantly impacted mortality.21 Broader integrated policies may be necessary for meaningful disparity reduction and long-term outcome improvement. High readmission rates are associated with overcrowded living conditions and reduced social connectedness.21,22 These factors correlate with higher regional readmission rates, indicating that community-level SDOH significantly influences patient recovery and care quality.23 Long-term outcomes, such as mortality, are also impacted by SDOH. Factors including unemployment, low SES, limited education, and social isolation correlate with worse overall and cancer-specific survival rates.24 Patients experiencing cardiac arrests in low-income, predominantly Black neighborhoods exhibit lower post-discharge survival rates due to restricted access to follow-up care and community resources.25 Policy interventions, including Medicaid expansion, have improved preventive care utilization and reduced mortality, especially among non-Hispanic Black populations, highlighting the potential of targeted policy actions to address health disparities.26,27 The effects of SDOH on increased readmissions and delayed care can negatively impact patient experience, which is a national quality imperative.28
Conclusion
Social determinants of health (SDOH) significantly influence every aspect of the patient’s healthcare journey, from initial access to treatment quality and post-discharge recovery. Structural conditions like economic inequality, policy frameworks, and neighborhood environments directly contribute to delayed care, reduced treatment quality, higher readmission rates, and increased mortality. Addressing these determinants through comprehensive systemic interventions reduces disparities and enhances patient outcomes. Recognizing and addressing SDOH can help healthcare systems deliver equitable and inclusive care, ultimately improving long-term health outcomes for vulnerable populations.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest
Corresponding Author
Farzana Hoque, MD, MRCP, FACP, FRCP,
Associate Professor of Medicine,
Saint Louis University School of Medicine,
1201 S Grand Blvd, St. Louis, MO 63104
Email: farzanahoquemd@gmail.com