Background
Strongyloides stercoralis is a parasitic infection endemic to sub-tropical areas of the world. Many communities, particularly within the United States, are becoming increasingly diverse and international. History of international travel has become increasingly common in a world with ongoing globalization. As infection can remain asymptomatic for years, Strongyloides infection should be considered for individuals with even a remote travel history. Since Strongyloides infection can persist over decades,1 some of the well known findings such as eosinophilia can wax and wane, making it difficult for lab findings to strongly indicate the presence of parasitic infection.1 Case reports have detailed a range of gastrointestinal findings associated with Strongyloides, ranging from mucosal edema and gastric ulcers to colonic ulcerations and peudopolyps.2 Thus, recurrent gastrointestinal symptoms in a patient with risk factors such as any travel to endemic regions should prompt evaluation for Strongyloides infection. Furthermore, Strongyloidiasis has been found even in the southeastern United States, meaning that an index of suspicion may be warranted even without travel outside of the country.3 We present a case of a patient where there was a delay in consideration of Strongyloidiasis that was ultimately diagnosed on colonoscopy and endoscopy after repeated contact with the healthcare system. This case highlights the importance of a high suspicion for Strongyloidiasis even in the absence of persistent eosinophilia or recent travel.
Case Presentation
A 71-year-old woman with a past medical history of type 2 diabetes mellitus and diverticulosis presented with abdominal pain, intermittent cough, nausea, vomiting, and weight loss. The patient described postprandial emesis associated with an epigastric burning sensation and warmth. She had lost 10 pounds over the last year and reported foul smelling stool, though denied hematochezia or melena. She had been seen in the Emergency Department (ED) three times over the last year for these symptoms and was diagnosed with diverticulitis and gastritis, and was sent home on antibiotics. Antibiotic treatments included a course of ciprofloxacin and metronidazole, and later a course of amoxicillin/clavulanic acid. The patient’s symptoms persisted despite the antibiotic treatments. The presumptive diagnoses of gastritis and diverticulitis remained as the patient waited for outpatient endoscopy and colonoscopy. Though plans were made by the ED for outpatient imaging, the patient was unfortunately lost to follow up. She presented for this hospitalization due to persistent symptoms and new weight loss. At home, she was taking medications for chronic hypertension and Type 2 diabetes, including amlodipine, aspirin, atorvastatin, glipizide, lisinopril, metformin, miglitol and sitagliptin. Her most recent colonoscopy was ten years prior, which the patient reports showed benign polyps though no formal colonoscopy report was available. Notably, the patient reported travel to Central America the previous year. She was born in Central America and had returned several times throughout the years.
On arrival, she was afebrile, hemodynamically stable, and resting comfortably on room air. On exam, she had diffuse tenderness throughout the abdomen, worse in the epigastrium, with no guarding, rigidity or rebound tenderness. There were no dermatologic findings on skin examination. Computed tomography of the chest, abdomen and pelvis with contrast showed mural wall thickening involving the transverse colon which persisted in comparison to imaging during a prior ED visit. Her initial labs demonstrated white blood cell count 7.5 x10^9/L (ref: 4.5 to 11.0 × 10^9/L), hemoglobin of 12.2 g/dL(ref: 12.1 to 15.1 g/dL ), Eosinophils of 5.5% (ref: <7%) with absolute eosinophil count of 400 per μL of blood (ref: 400-500 per μL of blood). She was admitted to the medicine service for further evaluation and workup of suspected malignancy given the imaging findings. On further chart review, the patient had waxing and waning mild eosinophilia for at least three years. Her maximum eosinophilia was 13.5% with an absolute count of 1400 per μL of blood on one of her previous ED visits, which was not commented on at that time. Though the patient did not have significantly elevated levels of eosinophils on arrival to the hospital, during her hospital stay the levels of eosinophilia fluctuated with a maximum of 8.3% eosinophils with absolute count of 700 per μL of blood.
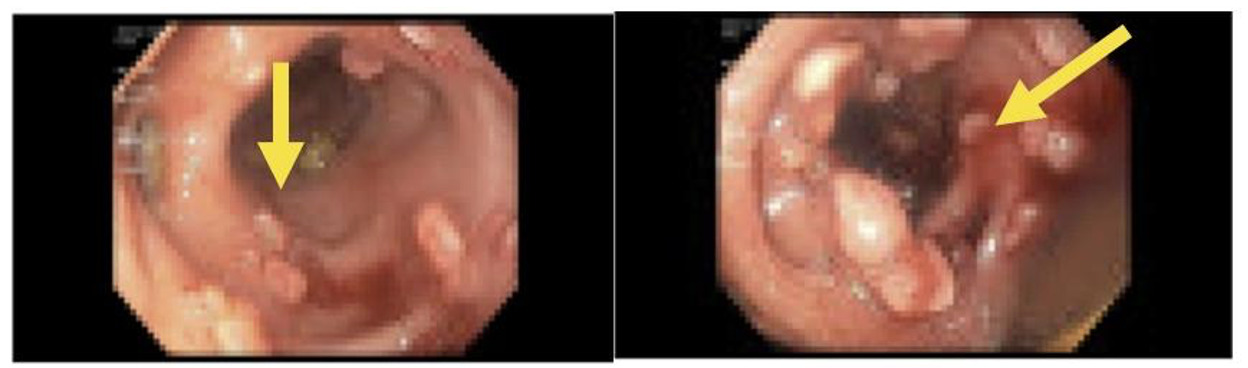
Gastroenterology was consulted immediately on admission, and esophagogastroduodenoscopy (EGD) and colonoscopy were performed on day two of hospitalization. EGD showed localized mild inflammation in the gastric antrum and body. The duodenal bulb had localized mild erythematous mucosa with no active bleeding. EGD showed gastritis and erythematous duodenopathy. On colonoscopy, the descending colon was found to have scattered moderate inflammation with erosions, erythema, loss of vascularity, and pseudopolyps as well as aphthous ulceration (Figure 1). Fecal calprotectin was ordered and was 1006.8 mg/kg (normal range less than 30-500 mg/kg). Erythrocyte Sedimentation Rate and C- reactive protein were 24 mm/h (normal range 0-20 mm/hour) and 12.11 mg/L (normal range < 4.0 mg/L) respectively. Stool polymerase chain reaction was negative for Giardia, Cryptosporidium, and Entamoeba histolytica.
_and_sigmoid_colon_(right)._findings_demonstrated_w.png)
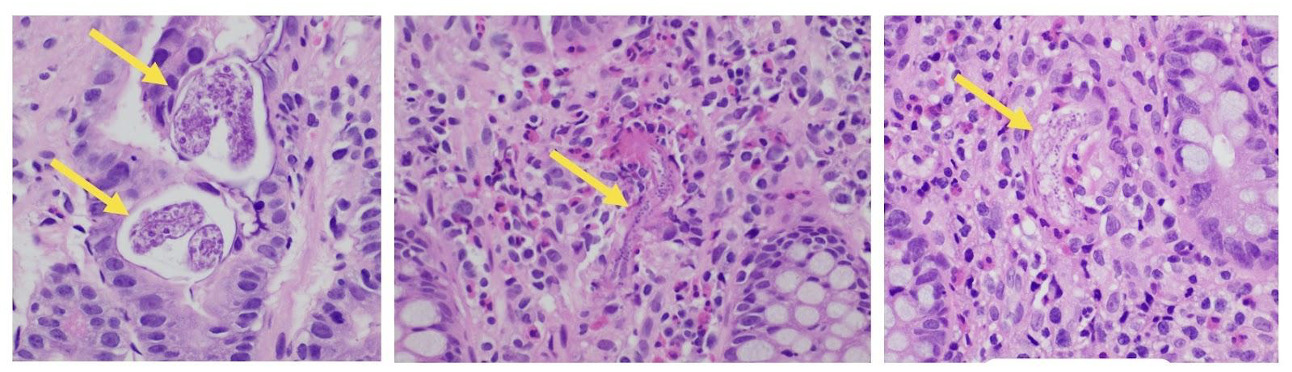
Biopsies were taken from areas of erythema and inflammation throughout the gastric antrum, duodenum, and colon, as well as from inflammatory polyps found in the descending and sigmoid colon. With Hematoxylin and Eosin (H&E) staining, the biopsies were negative for Helicobacter pylori but did demonstrate Strongyloides larvae in the gastric antrum, duodenum, and colon (Figure 2). Only after the pathology report showed infection was a Strongyloides IgG obtained, which was elevated at 2.6 IV (normal range below 1 IV). With infectious disease consultation, the patient was started on a two-week course of ivermectin for treatment of strongyloidiasis. A two week course was pursued in the setting of high infectious burden with colitis. In this case the patient was relatively stable, did not have evidence of hyperinfection, and thus received only ivermectin.She completed her two-week course of ivermectin and followed up with infectious disease outpatient, at which point her symptoms and eosinophilia resolved. Though the patient did not have a serum or stool test of cure, she had two follow up appointments with outpatient infectious disease clinic, one seven months later and one visit a year later. At these visits her eosinophilia was monitored, and it was decided to pursue stool ova and parasites only in the case of repeat symptoms.
_and_throughout_the_colon_(center_and_right)._eosinophi.png)
Discussion
The findings associated with Strongyloides infection can easily be mistaken for other diseases, as was the case with our patient. Weight loss, colonic wall thickening and general failure to thrive after multiple emergency room visits were mistaken as likely colorectal cancer. Once colon cancer was found to be less likely on colonoscopy, we began to suspect a new diagnosis of IBD. Had this patient been treated empirically with corticosteroids for IBD, there would have been a serious risk for disseminated Strongyloidiasis, which has a high rate of morbidity and mortality.1 Visualization with biopsy to clarify the diagnosis in this case was crucial given corticosteroid administration is contraindicated in Strongyloidiasis. This case highlights the importance of having a strong clinical suspicion for Strongyloidasis when patients have risk factors even when classic markers like eosinophilia are absent.
The life cycle of Strongyloides stercoralis infection begins with larvae in the soil infecting their host through direct skin contact. S. stercoralis enter the bloodstream and lymphatic systems, and migrate to the lungs. Migration continues when larvae are coughed up from the lungs and swallowed into the gastrointestinal tract where they mature and lay eggs in the intestinal submucosa.4 The clinical presentation of Strongyloidiasis often starts with nonspecific gastrointestinal symptoms such as diarrhea and vomiting. Additionally, cutaneous larva currens is a known dermatologic manifestation, and can be identified as a pruritic serpiginous rash which is pathognomonic for S. stercoralis infection.5,6 In chronic settings, eosinophilia may wane and patients may be asymptomatic for years or simply present with mild cough, gastrointestinal symptoms, or persistent dermatologic findings.7
Hyperinfection is an accelerated autoinfection cycle involving both the lungs and gut.8,9Disseminated strongyloidiasis, in contrast, involves the presence of Strongyloides outside of the skin, lungs and gastrointestinal tract involved in the general life cycle of S. stercoralis.10 For uncomplicated strongyloidiasis treatment, typically a regimen of ivermectin 200 micrograms/kg for two days is used.11 In patients who are hospitalized or critically ill, both ivermectin and albendazole (400mg twice a day for 3-7 days) are sometimes used together.8,9,11 Furthermore, in the setting of hyperinfection or disseminated disease Gram negative coverage against enteric bacteria may also be appropriate in addition to 200 µg/kg daily of ivermectin.7
Disseminated infection has a mortality rate as high as 68.5%,4 and can often be precipitated by corticosteroid administration in a patient with unknown Strongyloides infection.4,12 As corticosteroid medications are frequently used in the hospital by general internists to treat common conditions such as asthma exacerbations, Chronic Obstructive Pulmonary Disease (COPD) exacerbations, and Inflammatory Bowel Disease (IBD) flares, the ability to recognize the possibility of occult Strongyloides infection is crucial.8,9 In one case report, a patient was administered corticosteroids in the setting of presumed COPD and the patient died following hyperinfection.13 Finally, severe infection is also associated with other conditions that compromise the immune system, such as HTLV-1 infection, transplantation, or immunosuppresive medications like rituximab.8,9
One of the items on our differential for this patient was a new diagnosis of IBD. Though IBD generally presents earlier in life, it can occur at any age and there may even be a second peak in incidence in late adulthood.14,15 Visual findings on colonoscopy can appear quite similar in Strongyloidiasis and IBD. For example, strongyloidiasis can present with a skip pattern of inflammation on colonoscopy, sparing the rectum, with preserved crypt architecture and preserved goblet cell function, which can also be seen as IBD.8,9 The diagnosis of Strongyloides is often completed with serologic tests or testing for stool ova and parasites. In the absence of suspected hyperinfection, general practice recommends use of serological testing for screening.8,9 Stool evaluation is often reserved for cases of suspected hyperinfection in which the parasite burden is expected to be high.8,9 Because many patients at risk for disseminated infection are functionally immunocompromised, serologic testing is thought to be less accurate in disseminated infection.8,9 In our case, neither serologic testing nor stool evaluation were performed because the diagnosis was based on the pathology findings from colonoscopy, which is considered to be a definitive form of diagnosis.8
Conclusion
The gastrointestinal features of Strongyloides infection have primarily been documented in case-series reports. This case report demonstrates a rare example of non-disseminated Strongyloides infection presenting as ulceration and pseudopolyp formation on colonoscopy. Parasitic infections such as strongyloidiasis are often not considered in differential diagnoses in non-endemic regions such as the Northeastern United States. However, given our global population with a high prevalence of travel abroad and the chronic nature of parasitic infections like strongyloidiasis , this case highlights the importance of thorough travel histories and screening even outside of areas traditionally considered endemic for infection. Our case report provides an example of the gastrointestinal findings of non-disseminated Strongyloides infection as well as the necessity to obtain a thorough travel history and consider chronic parasitic infection prior to further treatment of other presumed conditions.
Disclosures/Conflicts of Interest
No disclosures or conflicts of interest to report
Corresponding author
Victoria P Angenent-Mari, B.S.
Warren Alpert Medical School of Brown University
Providence, RI 02906
Email: victoria_angenent-mari@brown.edu