Background
A discharge summary is a comprehensive medical document of a patient’s hospitalization and communicates essential information to subsequent care providers. It typically includes information such as admission diagnoses, hospital course, procedures and treatments during the hospitalization, discharge diagnoses, discharge medications, pending test results and recommendations for follow-up care.1 This document functions as a critical handoff, ensuring continuity of care and minimizing the risks associated with care transitions from the hospital to the outpatient settings.2
While timelines of discharge summary completion vary by institution, timely completion and transmission of discharge summaries, ideally within 24 to 48 hours of discharge, are widely recognized as best practice to support safe care transitions.3 Studies have found that discharge summaries completed within seven days are associated with reduced 30-day readmission rates. For example, delayed discharge completion (after seven days) was significantly associated with an increased risk of 30-day readmission in a study of over 140,000 discharges, reinforcing the importance of timely documentation.4
The widespread transition from paper records to electronic medical records (EMRs) in healthcare following the 2009 Health Information Technology for Economic and Clinical Health (HITECH) Act has created some standards with discharge summary documentation and accessibility to outpatient clinicians.5 It also helped eliminate errors that occurred with inconsistent terminology and illegible handwriting from paper records that were hand-written.6 However, variability in discharge summary quality and timeliness to completion persists, despite these digital advances.7
Importantly, the impact of discharge summary timeliness on patient outcomes such as readmissions remains under investigation. Some studies suggest that delayed discharge summary documentation can fragment care and increase risk of readmission,4,8 while others highlight a broader role for discharge summaries in improving medication reconciliation, patient education, and outpatient care coordination.1,7 Each of those components are critical in the patient transition process from inpatient to outpatient care.1 The utility of discharge summaries also depends on their quality, or more specifically their clarity and content, which can influence clinician satisfaction and a patient’s follow-up care.9
In the United States, transitions of care have become a focal point of national quality initiatives. Programs by the Centers for Medicare & Medicaid Services (CMS), such as the Hospital Readmissions Reduction Program (HRRP), directly link financial reimbursement to readmission rates and effective discharge practices.10 Similarly, the Hospital Value-Based Purchasing (VBP) Program ties hospital reimbursement to performance metrics including care coordination and patient experience, emphasizing the significance of clear, effective discharge communication.11
The discharge summary, while often overlooked in broader policy discussions, plays a pivotal role in supporting these quality objectives. Effective discharge summaries are central in ensuring continuity of evidence-based care as they provide crucial clinical details to outpatient clinicians, specialists, home health agencies, skilled nursing facilities, and case managers during transitions between care settings.10,12 Inadequate or delayed discharge summaries compromise coordination, increase healthcare costs and negatively impact patient trust and satisfaction.7,12
As healthcare shifts toward value-based purchasing and accountable care organizations (ACOs), the importance of high-quality discharge documentation continues to grow. Moreover, CMS’s patient experience surveys (HCAHPS) highlight the importance of clear, culturally sensitive, and respectful communication, which is critical not only for patient empowerment and trust but also for reimbursement outcomes.13,14 Effective communication in discharge summaries has also been shown to reduce readmissions and decrease healthcare utilization, reinforcing the humanistic value of them.7
This review aims to examine existing literature on discharge summary completion time and discharge summary quality, with a focus on measurable outcomes such as hospital readmissions, follow-up adherence and clinician satisfaction. We also highlight evidence gaps and identify areas of opportunity for future quality improvement or research initiatives.
Methods
Using the PRISMA guidelines, we conducted a structured literature search to evaluate the association between discharge summary completion timeliness, quality, and measurable patient outcomes. Searches were performed in PubMed and Google Scholar for peer-reviewed articles written in English published between January 2010 and June 2025. The 2010 start date was chosen to reflect the increasing adoption of EMRs in clinical settings, particularly in the USA.
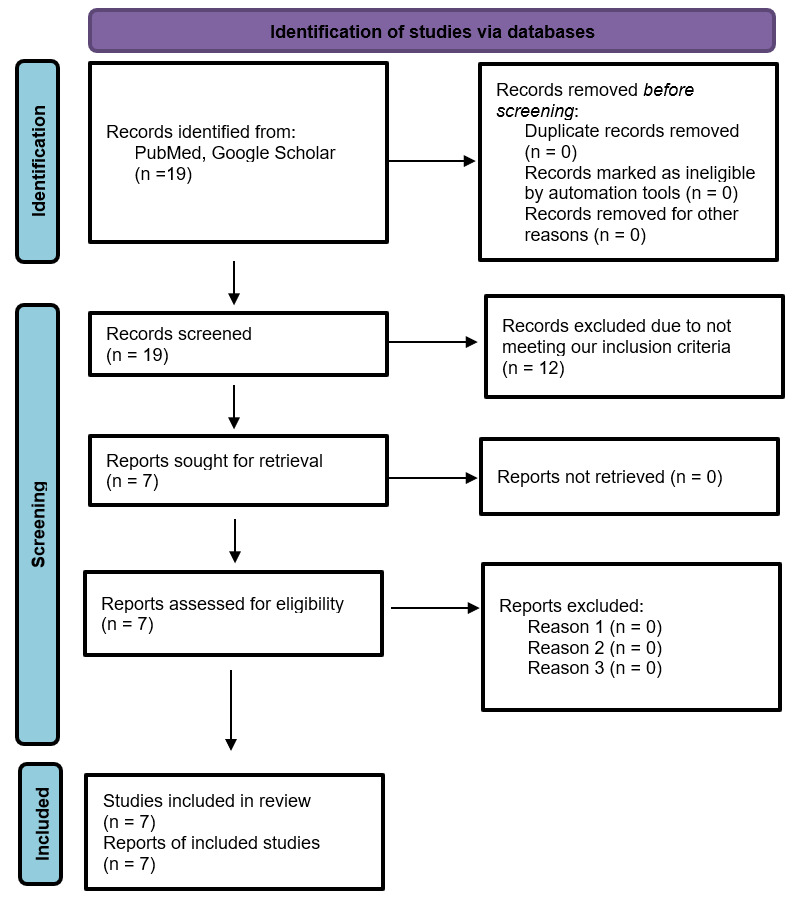
We used search terms combining keywords such as “discharge summary + completion time,” “discharge summary + quality.” Only studies involving adult patients (aged ≥ 18 years) were included. Titles and abstracts were screened for relevance and to assess for eligibility. Studies were included if they assessed either the timing of discharge summary completion or the quality of discharge summaries in relation to clinical or operational outcomes. Those eligible full-text articles were reviewed in detail (Figure 1).

Results
19 studies were reviewed, but a total of 7 articles met our inclusion criteria: 3 focused primarily on discharge summary timeliness and 4 on discharge summary quality (Table 1).
Timeliness of Discharge Summary Completion
Timeliness was found to have a direct correlation with patient outcomes, particularly in reducing hospital readmissions. Li et al. conducted a retrospective analysis of over 16,000 patients and observed that the absence of a discharge summary was associated with a 79% increase in 7-day readmissions (p<0.001) and a 37% increased risk of readmission within 28 days (p<0.001). If aged over 80 years, there was an 8% increase in 7-day readmission rate and 18% increase in 28-day readmission risk. If aged less than 80 years, the absence of a discharge summary was associated with a 127% increase in readmission rate within 7 days (p<0.001) and a 55% increase within 28 days (p<0.001) after discharge.4
Similarly, Lewis et al. reviewed 109 patients discharged from a large academic center and found that discharge summaries completed more than 7 days post-discharge when compared to <72 hours were significantly associated with significantly higher 30-day readmission rates (p=0.04). Interestingly, there was no statistical significance for readmission for discharge summaries completed between 72 hours and 7 days compared with <72 hours (p=0.44).15
Hoyer et al. analyzed 87,994 discharges at Johns Hopkins and found that 43% of readmitted patients did not have a completed discharge summary at the time of rehospitalization. They identified a dose-response relationship: for every three-day delay in discharge summary completion, the odds of readmission increased by 1%, independent of age, gender, illness severity, or clinical service (e.g., surgery, oncology). These findings highlight how delays in discharge summary generation can compound risk, particularly in complex, multi-specialty environments.8
Quality of Discharge Summaries
In addition to timing, the quality of discharge summaries was repeatedly cited as critical to safe transitions. Horwitz et al. found that discharge summaries completed in a timely fashion were significantly more likely to contain key post-discharge information, such as pending test results, follow-up instructions, and medication reconciliation. Late or poorly constructed discharge summaries, by contrast, lacked essential details, reducing their utility to outpatient providers.7
Several interventions aimed at standardizing discharge summary content were shown to improve documentation quality. Scarfield et al. implemented a 10-point discharge template across acute medical wards at a hospital in the United Kingdom, resulting in a marked increase in documentation compliance from 55% to 97% in 7 months. Beyond improved completeness, clinicians also reported that the discharge summaries became easier and quicker to write, improving workflow efficiency.16
Similarly, Fazal et al. implemented a standard template at a tertiary care hospital in Pakistan and observed notable improvements in discharge summary completeness. For example, allergy documentation rose from 3% to 51% (p<0.05), and documentation of past medical history, secondary diagnoses, and follow-up plans all improved. This intervention demonstrates that standardized templates can be adapted across diverse healthcare settings and lead to measurable gains in clinical documentation.17
However, the relationship between discharge summary quality and timeliness is not always linear. Goldszmidt et al. found that setting a 48-hour goal for discharge summary completion across six inpatient teams led to improved timeliness (from 62% to 75% completion over 1 year), but with variable effects on documentation quality. Challenges included increased workload pressures, reduced flexibility in content detail, and concerns over assigning documentation to trainees with less experience in writing them. These findings emphasize that while timeliness goals are important, they must be balanced against cognitive workload and content fidelity.3 Overall, the findings suggest that both the timeliness and quality of discharge summaries are critical, and optimizing both requires systemic changes to workflows, staffing models, and EHR tools.
Discussion
Our review demonstrates that both the timeliness and quality of discharge summaries are important for the transitions of care. Discharge summaries completed within seven days of discharge are consistently associated with lower readmission rates. In parallel, high-quality discharge summaries that contain essential clinical details, such as medication changes, clear follow-up recommendations, improve continuity, and post-discharge outcomes. Inadequate or delayed discharge summaries, by contrast, contribute to fragmented care and avoidable harm.
The discharge summary serves as an important tool for handoff between inpatient and outpatient care teams for patients. When this is delayed or of low-quality, outpatient clinicians are often left to reconstruct a patient’s hospital course without all of the necessary context. Studies by Li et al. and Hoyer et al. suggest that failure to complete discharge summaries promptly can directly contribute to rehospitalizations.4,8 In this way, discharge documentation is not simply an administrative task, but a safety-critical process that affects clinical decision-making and care plan adherence.
Efforts to improve discharge summary timeliness and quality have increasingly focused on structured discharge summary templates and training. Standardized discharge summaries, such as those implemented by Scarfield et al. and Fazal et al., improve discharge summary content consistency while ensuring completeness.16,17 Additionally, embedding discharge summary education into learning curricula have been shown to improve quality and physician confidence. Such training is particularly important for early-career clinicians tasked with writing complex discharge summaries during busy inpatient rotations.
Many institutions struggle to balance competing demands of ensuring timely discharge summary completion while maintaining quality. Goldszmidt et al., reported that setting strict deadlines (e.g., 48-hour discharge summary completion targets) improved timeliness, but sometimes compromised the quality of discharges, particularly when discharge summaries were delegated to more junior members of the team or completed with minimal supervision from more experienced writers.3 These findings reflect the broader challenge of the pressure to meet operational metrics while not overshadowing the clinical purposes of the discharge summary. Institutions must weigh whether discharge summary completion time alone is a meaningful marker of discharge summary quality.
Emerging technologies, such as artificial intelligence (AI) and natural language processing, offer promising avenues to support discharge summary creation.18 In a cross-sectional study of 100 patients from a deidentified database of patients admitted to a hospital medicine service, large language model (LLM)-generated discharge summaries were compared with those written by clinicians.19 The discharge summaries were rated comparable in overall quality.19 However, LLM-generated discharge summaries were more succinct but had a higher proportion of potentially low-harm errors, mostly errors of omission.19 These findings suggest that AI platforms can potentially extract relevant data and information from the EHR and generate discharge summaries to potentially reduce documentation burden and ensure both quality and efficiency. Future work should evaluate how AI can enhance, not replace, clinician judgement, especially in capturing clinical reasoning and individualized recommendations. In addition, more rigorous, multi-institutional research is needed to explore the long-term impact of discharge summary interventions on patient-centered outcomes. Incorporating feedback on receivers of discharge summaries and patients themselves could strengthen the relevance and usability of these discharge summaries in real-word settings.
These findings also suggest that discharge summary improvements may have downstream effects beyond readmission metrics. For example, enhancing documentation quality could reduce provider cognitive load during follow-up appointments, support team-based care by clarifying roles and responsibilities, and even inform public health surveillance efforts that rely on accurate documentation of diagnoses and care plans.
Moreover, discharge summaries are an educational opportunity. For trainees and early-career clinicians, they provide a structured method to synthesize complex hospital courses and communicate them clearly, skills that are foundational to good clinical reasoning. A randomized study of internal medicine interns demonstrated that a targeted discharge summary curriculum, especially when paired with individualized feedback from attending physicians, significantly improved the quality, organization, and readability of discharge summaries.20 Embedding structured feedback, experienced reviewers from attending physicians, and checklist-based prompts into the discharge summary workflow may enhance not only the discharge document’s utility but also the clinician’s learning curve. Such educational interventions can foster practice-based learning and systems-based thinking, ultimately benefiting both trainees and patient care.
This article is subject to several limitations. First, the literature base remains modest, with many studies using observational designs, single-center data, or convenience sampling. This limits the generalizability of findings across settings with different EHR platforms, staffing models, or institutional cultures. Second, while we attempted to focus on articles within the United States to ensure contextual relevance, valuable insights from international health systems may have been excluded. Third, we were unable to quantitatively assess effect sizes or conduct a formal meta-analysis, as our objective was to synthesize qualitative and narrative findings from diverse study designs. As such, future systematic reviews on this topic may benefit from incorporating gray literature, direct patient feedback, and mixed-methods evaluations to better understand the impact of discharge summaries across multiple dimensions of care.
Conclusions
Discharge summaries are a vital bridge between inpatient and outpatient care, and their timeliness of completion and quality are both critical for improving patient outcomes and enhancing care continuity. While no single timeframe for discharge completion window guarantees better outcomes, aiming to complete discharge summaries within seven days may be helpful in reducing readmission risk. It is essential to weigh the content quality in the discharge summary with timeliness as well. Using structured templates and training to ensure high-quality discharge communication remains a fundamental strategy in delivering safer, more coordinated patient care. Exploring technological tools such as artificial intelligence to enhance efficiency without sacrificing quality. Rigorous studies are needed to establish causal relationships and to evaluate the sustainability and scalability of discharge summary improvement initiatives.
Disclosures/Conflicts of Interest
None
Corresponding author
William C. Lippert, MD, MPH
Associate Professor, Internal Medicine
Wake Forest University School of Medicine
1 Medical Center Boulevard Winston – Salem, NC 27157
Telephone: 336-713-5215
Fax: 336-716-0030
Email: william.lippert@wfusm.edu