Background
Hemophagocytic lymphohistiocytosis (HLH) is a potentially fatal hyper-inflammatory syndrome, often secondary to an underlying trigger in adults. Among secondary causes, malignancy-associated HLH carries the poorest prognosis, though association with solid tumors is rare. In adults with suspected secondary HLH and unrevealing infectious/rheumatologic evaluation, clinicians should evaluate for occult malignancy, including solid tumors with marrow involvement. We describe a patient with metastatic carcinoma of probable colorectal origin who presented with secondary HLH as the initial manifestation.
Case presentation
A 40-year-old Asian male presented to his primary care physician with a two-week history of fatigue, intermittent fevers, haematochezia, constipation, and poor appetite, accompanied by a 5-pound weight loss. He has a past medical history of anxiety, depression, dyslipidemia, and prediabetes, and takes a multivitamin at home. He has a 5-pack-year smoking history and quit smoking 15 years ago. He does not consume alcohol. He has no family history of colon cancer and never had a colonoscopy. He was initially treated with antibiotics for presumed colitis but returned in 5 days with acute-onset low back pain, unrelated to trauma and unrelieved by analgesics. An X-ray of the lumbar spine showed degenerative changes at L5–S1. His haematochezia persisted, and over the following three weeks, his back pain worsened and fevers continued. Outpatient labs revealed leucocytosis of 19 x 109/L (reference range [RR]: 4-11 x 109/L) and an elevated erythrocyte sedimentation rate of 99 mm/hr (RR: 0-15 mm/hr), raising concern for discitis, and he was referred to the emergency department (ED).
In the emergency department, he was hemodynamically stable but febrile, with a temperature of 100.9°F. Laboratory testing was significant for an elevated WBC count of 16.9 x 109/L, hemoglobin of 11.1 g/dL (RR: 13-18 g/dL), platelets of 267 x 109/L (RR: 150-450 x 109/L), ferritin of 1952 ng/mL (RR: 30-322 ng/mL), and alkaline phosphatase of 1380 U/L (RR: 46-116 U/L). CT abdomen and pelvis with intravenous (IV) contrast revealed multiple scattered hypoattenuating liver lesions, diffuse sclerotic changes in the vertebral bodies, femurs, and pelvis with a compression deformity involving the 8th thoracic vertebral body, and several subcentimeter retroperitoneal lymph nodes considered to be reactive. He was started on broad-spectrum antibiotics for sepsis presumed to be secondary to bacteremia from a gastrointestinal source in the setting of bleeding with subsequent hepatic and osseous seeding, manifesting as liver lesions and vertebral discitis/osteomyelitis, respectively.
The following day, he developed acute kidney injury (AKI) with decreased urine output and creatinine rising to 3.2 mg/dL (RR: 0.7-1.2 mg/dL). IV fluids and oral tamsulosin were initiated with no improvement. Nephrology attributed his AKI to acute tubular necrosis (ATN) from sepsis, antibiotics, recent non-steroidal anti-inflammatory drug (NSAID) use, and exposure to IV contrast. Blood cultures drawn at admission did not grow any organisms. A non-contrast CT chest was obtained for new onset dyspnea that revealed diffuse sclerotic bone lesions and bilateral patchy ground-glass opacities, concerning for multifocal pneumonia versus pulmonary edema. MRI abdomen was concerning for metastatic disease, and hence, tumor markers were sent. Carcinoembryonic Antigen (CEA) was elevated at 366.6 ng/mL (RR: 0-5 ng/mL), beta human chorionic gonadotropin at 3.4 IU/L (RR: <1.4 IU/L), and prostate-specific antigen (PSA) was normal. His renal function continued to worsen, and 4 days later, he developed uremic encephalopathy requiring emergent intubation for airway protection. He was transferred to the intensive care unit (ICU) on day 6 of admission and was initiated on hemodialysis.
During admission, his haemoglobin gradually declined, dropping from 8.4 to 6.7 g/dl on day 8, prompting transfusion of one unit of packed red cells. Platelets also decreased to 123 × 10^9/L. On day 9, he spiked a fever of 102.2°F. Laboratory testing revealed elevated triglycerides of 371 mg/dL (RR: 30-150 mg/dL), fibrinogen of 984 mg/dL (RR: 173-454 mg/dL), and ferritin of 8289 ng/mL in addition to progressive anemia and thrombocytopenia. An initial bone marrow aspiration was a dry tap and a core bone marrow biopsy was obtained. Bronchoscopy with bronchoalveolar lavage (BAL) showed 70% neutrophils and airway secretions, suggesting an inflammatory process, in the setting of an unremarkable infectious and autoimmune workup. Given high suspicion for HLH, he was started on dexamethasone on day 10 of hospitalization. His soluble interleukin-2 receptor (sIL-2R) level was sent, which returned elevated 2 days later at 7741.1 pg/mL (RR: 175.3-858.2 pg/mL).
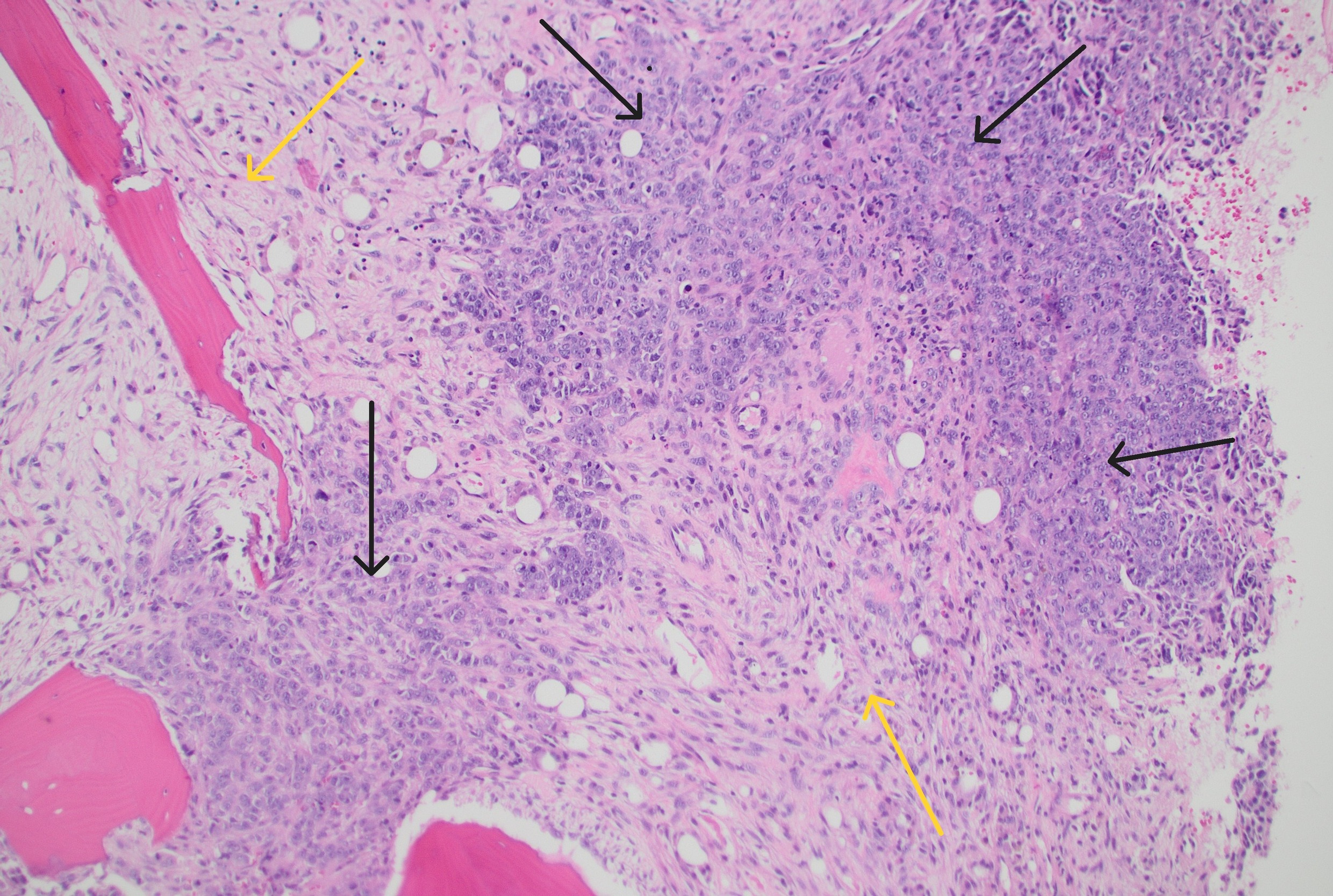
On day 13, his bone marrow biopsy returned positive for metastatic poorly differentiated carcinoma replacing marrow spaces (Figure 1). Immunostaining was positive for CK20, CDX2, pancytokeratin, and negative for CK7, TTF-1, Napsin A, NKX3.1, GATA3, S100, CD30, OCT4 and SAL4, suggestive of colorectal cancer. Colonoscopy was deferred by consulting gastroenterologist due to his acute medical issues. Immunostaining for DNA mismatch repair (MMR) deficiency showed intact MLH1, MSH2, PMS2 and MSH6 expression. He briefly required continuous renal replacement therapy (CRRT) but was eventually extubated to high-flow nasal cannula on day 15. By day 17, his renal function had improved, and he no longer required CRRT. He was weaned to 2 L of oxygen via nasal cannula and transferred to the general medicine floors on day 22.

The patient was deemed ineligible for chemotherapy by a consulting oncologist due to poor performance status, and his prognosis was estimated to be less than 3 months. He remained on dexamethasone dosed per HLH-2004 protocol. His hospital course was complicated by anxiety, delirium, and pain. On day 46, he developed respiratory distress and worsening hypoxia, requiring high-flow nasal canula, and his code status was changed to do not resuscitate (DNR) and do not intubate (DNI), with bilevel positive airway pressure (BiPAP) permitted. Despite temporary improvement, he subsequently developed pulmonary edema and increasing oxygen requirements and was treated with diuretics and antibiotics for suspected aspiration pneumonia. On day 54, he developed apnea and asystole, passing away shortly after.
Discussion
Hemophagocytic lymphohistiocytosis is a hyper-inflammatory condition that can lead to multi-organ failure and death if not promptly treated. It is classified into primary HLH, a familial disease seen in the pediatric population, and secondary HLH, which is more common in adults. Infections, malignancies, and autoimmune conditions are the most common triggers for secondary HLH. The incidence of all forms of HLH in England in 2018 was estimated to be 4.2 cases per million.1 The prevalence of secondary HLH is not well known, and the condition still remains underdiagnosed across the globe.2 A retrospective study analyzing the trends of adult HLH admissions from 2006 to 2019 in the USA reported a statistically significant annual percentage change (APC) of 25.3%, suggesting a significant increase in incidence of HLH per 1,00,000 population.3 When initial workup for secondary HLH is unrevealing, it is important to re-evaluate for occult tumors, infections, or rheumatological conditions.4
Hematological malignancies are the most common triggers for malignancy-associated HLH. Ramos-Casals M et al. reviewed 2197 published case reports of adult HLH and found that only 32 cases were secondary to solid tumors.5 Solid tumors account for 3% of malignancy-associated HLH.6 This rare condition is usually seen in cases with metastatic disease, typically with bone marrow involvement and with underlying aggressive histologies such as germ cell tumors or melanoma.7 Irrespective of the etiology of HLH, corticosteroids are used in the initial treatment regimen, and dexamethasone is the preferred steroid when central nervous system involvement is suspected as it has better penetration through the blood brain barrier compared to prednisone or prednisolone.5
HLH is characterized by excessive inflammation that develops from dysregulated positive feedback loops between CD8+ T-lymphocytes and macrophages, which leads to increased circulating cytokines, causing inflammatory cells to infiltrate tissues and consequent multi-organ damage.7 Secondary HLH in adults is triggered by highly immunogenic triggers namely certain infections, autoimmune conditions or cancers.2 This patient presented with symptoms and signs suggestive of an infection involving his thoracic vertebra. However, infectious work up returned negative, and on day 10 of hospitalization, he was diagnosed with HLH as he met 5 out of 8 HLH-2004 criteria namely- fever, cytopenias, hypertriglyceridemia, hyperferritinemia, and elevated soluble IL2R levels. Adult HLH patients often have ferritin levels >7,000–10,000 ng/ml. However, sIL-2R may have better diagnostic performance, with an AUC of 0.90 (95% CI 0.83–0.97) compared to ferritin (AUC 0.78, 95% CI 0.67–0.88). Taken together, sIL-2R may be a stronger diagnostic marker than ferritin in adults suspected of HLH.6 Hemophagocytosis may not be seen on bone marrow biopsy as it may take days to weeks for the pathological changes to be evident (as in our patient). Hence, absence of hemophagocytosis on histopathological evaluation should not delay treatment when the suspicion for HLH is high.8 Imaging did not reveal splenomegaly and NK cell activity was not checked.
Malignancy-associated HLH is a subtype of secondary HLH with the worst prognosis, partly due to poor survival from the underlying cancer.2 Our patient had secondary HLH triggered by metastatic poorly differentiated carcinoma of probable colorectal origin. Although colonoscopy could not be performed for direct visualization due to poor candidacy, the diagnostic reasoning supporting a colorectal primary is strong, particularly given the bone marrow biopsy immunophenotype (CK20+, CDX2+, CK7–) and elevated CEA level. The first step in treatment of malignancy-associated HLH involves targeting hyperinflammation with glucocorticoids, moderate dose etoposide with or without intravenous immunoglobulin followed by targeting the cancer itself once organ function improves.2 However, depending on the acuity of presentation, some patients receive only steroids due to concerns of myelosuppression from etoposide (as in our case), and others incorporate etoposide in chemotherapy regimens when possible.7
Based on our literature review, only two cases of malignancy-associated HLH presenting as the initial manifestation of colorectal cancer have been reported.9,10 In the first, the diagnosis of colorectal cancer was confirmed by colonoscopy,9 while in the second, it was established through immunophenotypic analysis of a metastatic lesion.10 To date, ours represents the third reported case of malignancy-associated HLH as the initial presentation of colorectal cancer, and the second in which diagnosis was achieved through immunophenotyping. Notably, our case was further complicated by an initial presentation that mimicked infection, resulting in a delayed diagnosis (Table 1). This case also underscores the importance of adhering to updated colon cancer screening guidelines to begin at 45 years of age, particularly in light of data demonstrating an increasing disease burden among persons below 50 years of age.11
In summary, HLH needs to be kept in mind as a differential diagnosis when patients present with features suggestive of an infectious process. HLH can be triggered by solid tumors, and an occult malignancy should be considered when initial evaluation for secondary HLH is unrevealing. This is so far the third reported case of malignancy-associated HLH as the initial presentation of colorectal cancer, and the second in which diagnosis was achieved through immunophenotyping of a metastatic lesion. Malignancy-associated HLH generally portends a poor prognosis in patients with colorectal cancer.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest
Corresponding author
Kavya Balusu, M.B.B.S
Resident Physician,
Department of Internal Medicine,
Rochester General Hospital,
1425 Portland Avenue,
Rochester, New York, 14621.
Email: kavyabalusu1998@gmail.com