A 63-year-old African American female presented with abdominal pain and multiple episodes of hematemesis and melena. The patient had a history of chronic kidney disease, alcohol use disorder, and deep venous thrombosis, not on anticoagulation, and status post inferior vena cava filter. Initial laboratory revealed normocytic anemia (hemoglobin: 5.8 g/dL), guaiac-positive stools, normal lipase levels, and normal liver function tests.
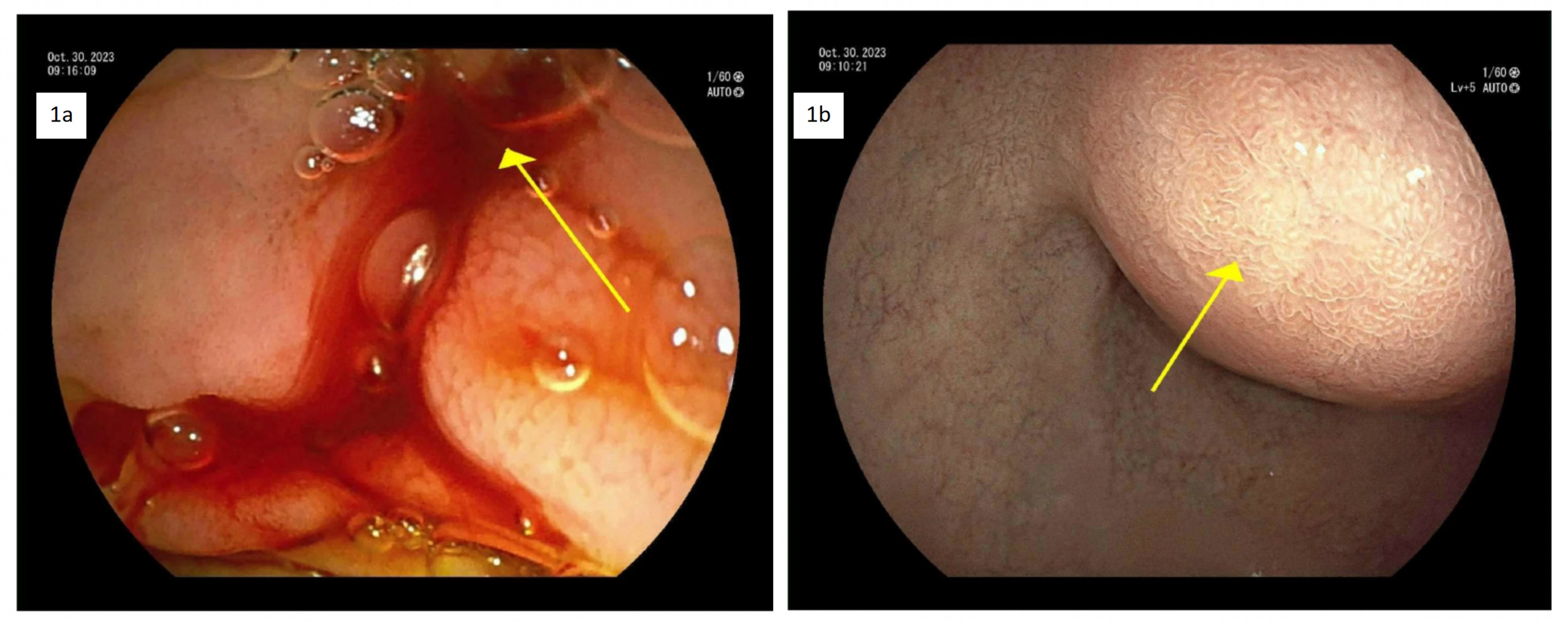
On day 1, the immediate management required 2 units (560 mL) of packed red blood cell transfusion. Further evaluation with a contrast Computed Tomography (CT) scan of the abdomen to identify the source of bleeding revealed a heterogeneous lesion along the pancreatic head and uncinate process, measuring approximately 4.1 x 3.7 cm. There were multiple enhancing foci along the mass-like structures, the largest measuring 1.6 x 0.9 cm. Similar lesions were noted in the pancreatic head and tail, suggesting sequelae of chronic pancreatitis. Gastroenterology was consulted. After stabilization, on day 2, the patient underwent upper gastrointestinal endoscopy (UGIE) with endoscopic ultrasound (EUS). The EUS showed findings suggestive of chronic pancreatitis with multiple cysts, and the UGIE showed active bleeding from the ampulla of Vater [Figure 1a] and subepithelial prominence of the duodenal bulb [Figure 1b], likely from the pancreatic pseudoaneurysm.
**_upper_gi_endoscopy_revealing_**_hemosuccus_pancreaticus_**_-_active_bleeding_from_.png)
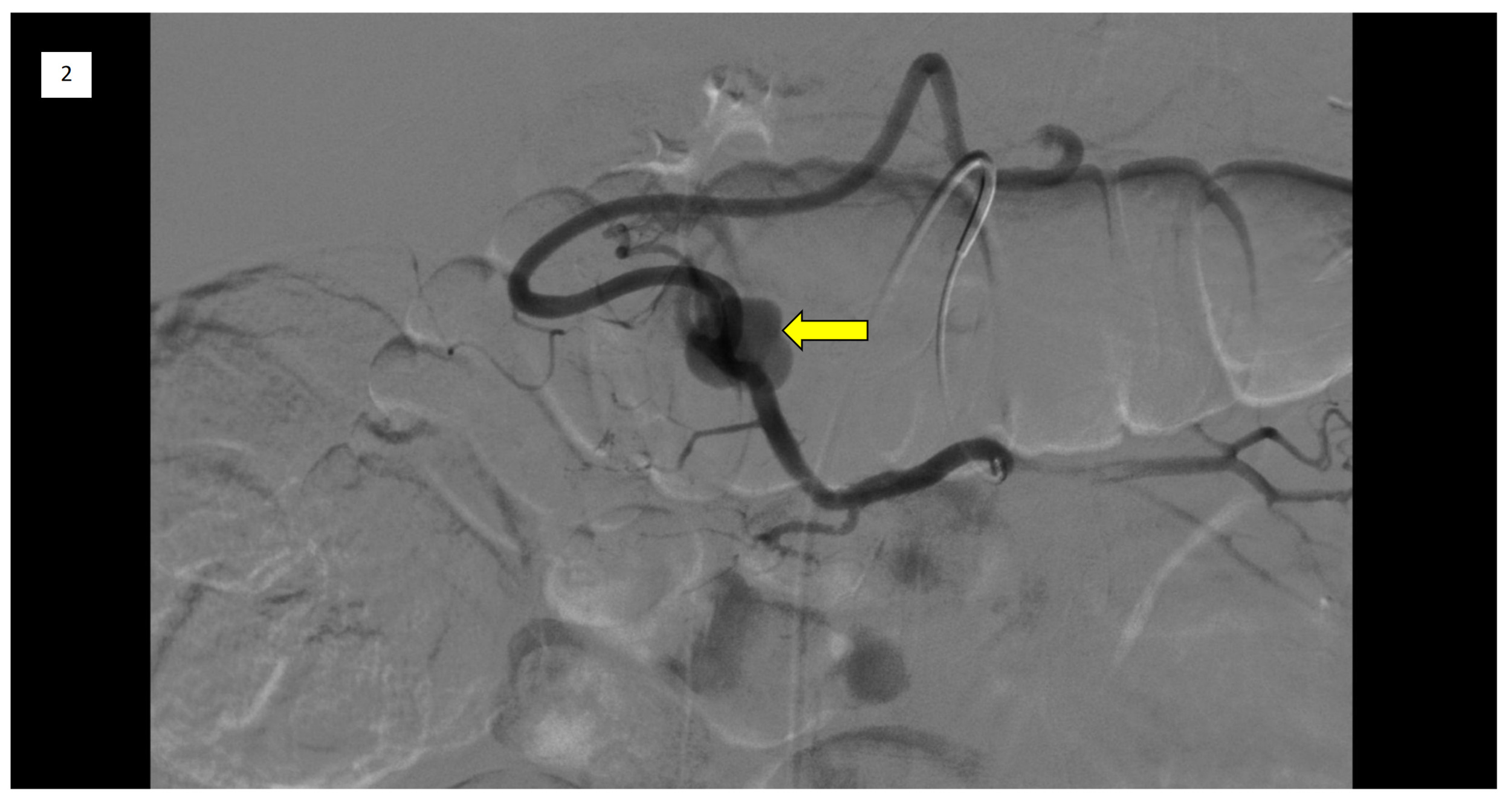
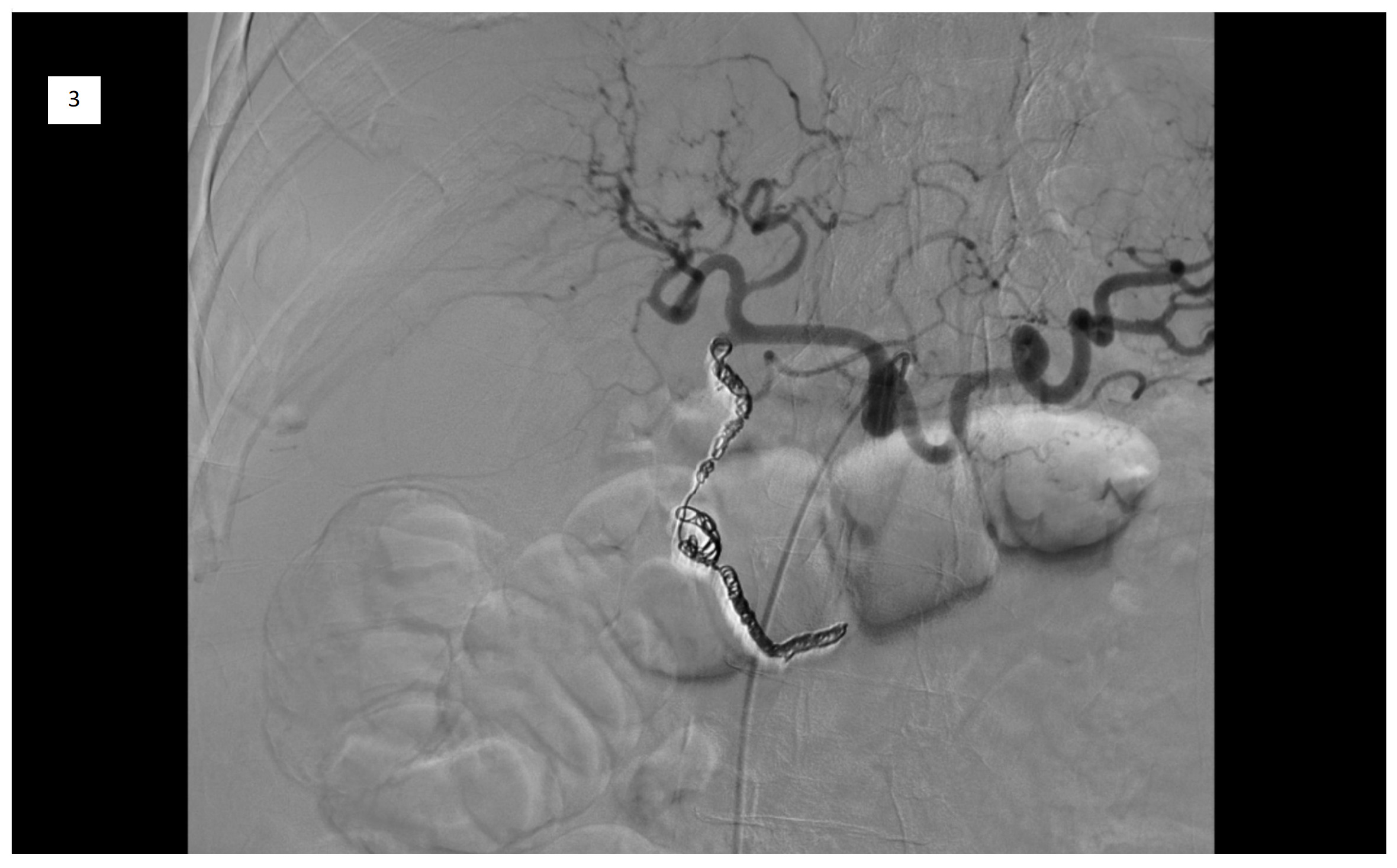
On day 2, an emergency Celiac artery angiography was performed by Interventional Radiology, which demonstrated a patent GDA with delayed and faint filling of a pseudoaneurysm centered in the GDA territory. The angiograms of the superior mesenteric artery (SMA) and the inferior pancreaticoduodenal artery (IPDA) demonstrated brisk filling of a large pseudoaneurysm in the GDA territory (Figure 2) and an additional, much smaller pseudoaneurysm more distally with a large feeding vessel from the IPDA. Subsequently, micro-catheterization of the SMA and retrograde catheterization of the proximal GDA were performed. Due to difficulties in deploying POD 6 and POD 4 coils, coil embolization was ultimately performed using multiple detachable and soft coils appropriately sized to the target vessels. Post-embolization angiography from IPDA demonstrated successful occlusion of the GDA and the large pseudoaneurysm, as well as that of large feeding vessels to the smaller pseudoaneurysm (Figure 3). A follow-up CT scan on day 3 confirmed resolution of the pseudoaneurysm and a stable hematoma.
_in_the_gastroduodenal_art.png)

Hemosuccus pancreaticus (HP) is a rare and potentially life-threatening cause of upper gastrointestinal bleeding.1 It is not easily diagnosed; hence it is often missed. It is described as a hemorrhage originating from the ampulla of Vater, passing through the main pancreatic duct toward the second portion of the duodenum.2 It could result from the rupture of a pancreatic pseudoaneurysm, which most commonly arises in the splenic artery (37.9%).2 Other arteries that may be involved include the gastroduodenal artery (21.8%) and, less commonly, the superior mesenteric artery, left gastric artery, and unnamed cystic wall vessels.2,3 Common associations include chronic pancreatitis (75.8%), acute necrotizing pancreatitis (12.6%), and recurrent acute pancreatitis (4.6%).3 Herein, we report a case of hemosuccus pancreaticus presenting with abdominal pain, multiple episodes of hematemesis and melena, diagnosed during upper GI endoscopy (UGIE). The bleeding originating from the ampulla of Vater into the duodenum was secondary to a ruptured pseudoaneurysm in the gastroduodenal artery (GDA) and the inferior pancreaticoduodenal artery (IPDA) and was successfully treated with retrograde coil embolization. This case highlights the diagnostic and therapeutic challenges of identifying and treating multiple pseudoaneurysms in HP, which necessitate multidisciplinary collaboration.
Hemosuccus pancreaticus presents diagnostic challenges due to its rarity, multiple causes, and ambiguous symptoms. Treatment might be impeded, especially in cases with intermittent bleeding, which delays the diagnosis.4 The diagnosis relies on clinical suspicion, imaging, and endoscopy. HP is more common in men and typically presents with epigastric pain with back radiation, accompanied by intermittent GI bleeding.3 Most commonly, the splenic artery is implicated, but other arteries, including the gastroduodenal, pancreaticoduodenal, and left gastric arteries, may also be involved.5 Pancreatic pseudoaneurysms are among the most common causes. Pseudoaneurysms carry a 37% risk of rupture and 90% mortality rate in the absence of treatment.6 Hence, being a potentially life-threatening condition, the knowledge of this rare entity and the provision of multidisciplinary and multimodal therapy are mandatory for the successful treatment.4
GDA pseudoaneurysm leading to HP requires early diagnosis and prompt management. Only 22 cases have described hemosuccus pancreaticus from the gastroduodenal artery pseudoaneurysm in the literature to date.7 Cases such as ours with multiple pseudoaneurysms are a diagnostic challenge, as direct visualization of active bleeding from the ampulla of Vater by endoscopy is seen in only 30% of patients.8 Expertise in abdominal vascular radiology is crucial for identifying and managing these lesions. CT angiography remains the gold standard in diagnosing HP.9,10 Arterial embolization is the first-line treatment for HP.8 It can facilitate hemostasis in an unstable hemodynamic setting, with overall low rates of post-intervention rebleeding.2 In patients with persistent hemodynamic compromise or failed embolization, surgical intervention should be considered. A timely consultation with the relevant specialists, along with a well-coordinated multidisciplinary approach, may lead to a favorable outcome.11
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding author
Sushrut Ingawale MD, DNB, MBBS
Department of Internal Medicine,
Quinnipiac University - Frank H Netter, MD School of Medicine/St. Vincent’s Medical Center
Email: drsushrutingawale@gmail.com