QUESTION 1: SHOULD PATIENTS WITH DIABETES STARTING GLP-1 RECEPTOR AGONISTS UNDERGO ROUTINE FIBROSIS RISK STRATIFICATION?
A 52-year-old man with long-standing type 2 diabetes mellitus (T2DM), obesity (BMI 36 kg/m²), and hypertension was followed in a primary care clinic for suboptimal glycemic control. He was initiated on a glucagon-like peptide-1 receptor agonist (GLP-1 RA), resulting in substantial weight loss and improvement in hemoglobin A1c. Over the following year, his liver enzymes remained mildly elevated but stable, prompting no further evaluation. Eighteen months later, he presented with ascites and upper gastrointestinal bleeding and was diagnosed with decompensated cirrhosis due to metabolic dysfunction–associated steatotic liver disease (MASLD). Retrospective review revealed that his fibrosis-4 (FIB-4) score had exceeded high-risk thresholds before GLP-1 therapy initiation, yet no fibrosis risk stratification had been performed.
A: This case illustrates a growing disconnect in contemporary metabolic care. GLP-1 RAs have become cornerstone therapies for obesity and T2DM.1 Large epidemiological studies report a prevalence of MASLD of up to 79% among individuals with both T2DM and obesity.2 Despite this substantial burden, noninvasive evaluation of liver fibrosis, the most important prognostic determinant in MASLD, remains inconsistently implemented in primary care and endocrine practice.1–3 Advanced fibrosis drives most of the liver-related morbidity and mortality, making early identification of high-risk patients essential.1
Professional societies recommend a stepwise approach to fibrosis risk assessment in at-risk populations, beginning with serum-based indices such as FIB-4, followed by vibration-controlled transient elastography (VCTE) or the Enhanced Liver Fibrosis (ELF) test when initial results are indeterminate or elevated.1,2 Magnetic resonance elastography (MRE) is the most accurate noninvasive imaging modality for fibrosis assessment and is often regarded as the reference standard, while liver biopsy remains the histologic gold standard. MRE may be particularly useful when VCTE results are indeterminate or technically limited.1 However, real-world implementation remains inconsistent. Many patients initiating GLP-1 RA therapy do so without baseline liver staging, reflecting persistent gaps in guideline adoption.
Although GLP-1 RAs and dual incretin agonists demonstrate improvements in steatohepatitis and, in some cases, fibrosis, therapeutic responses are variable and frequently incomplete.4 These agents should complement, rather than replace, structured fibrosis assessment. Identifying advanced disease remains critical for timely hepatology referral, portal hypertension screening, and hepatocellular carcinoma surveillance. Reliance on pharmacotherapy alone risks delayed recognition of cirrhosis until complications develop. Recent population-based data further emphasize the need to at least double the diagnostic rate of at-risk individuals through systematic implementation of noninvasive testing strategies, including serum fibrosis scores, liver elastography, and imaging modalities.3 Dependence on clinical suspicion or isolated liver enzyme abnormalities alone is insufficient and contributes to delayed diagnosis.3
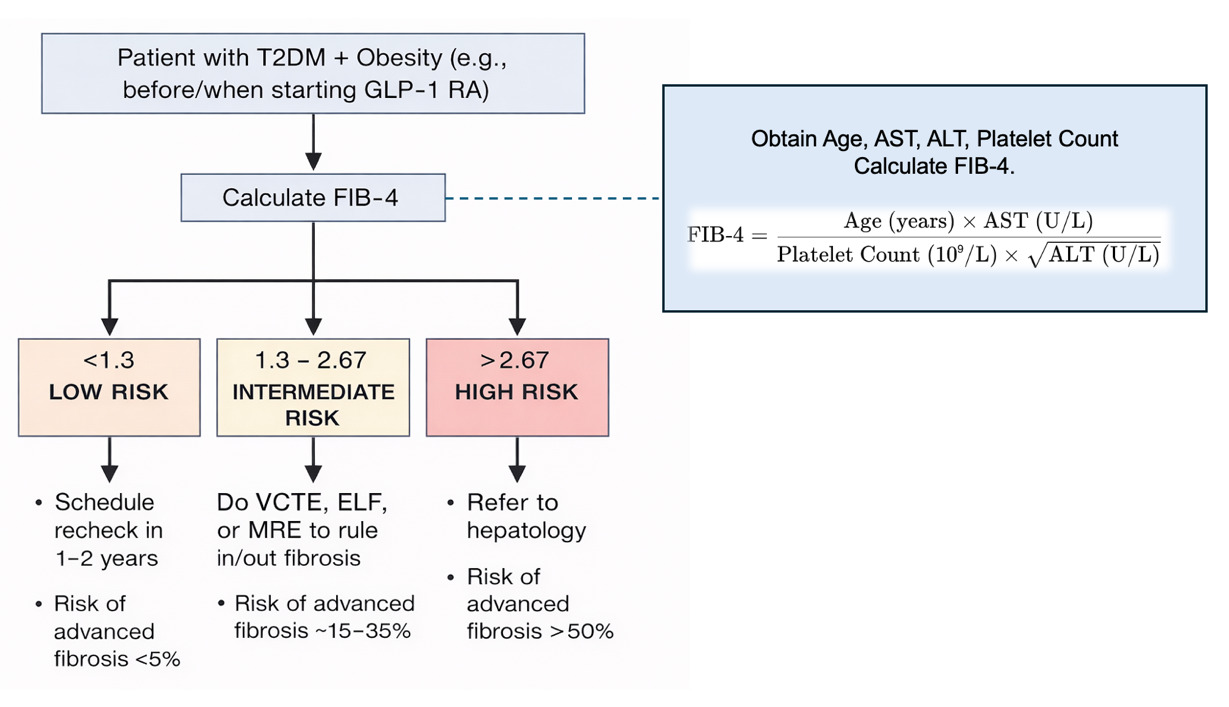
A practical solution is to embed MASLD screening into primary care and endocrine workflows at or before GLP-1 RA initiation (Figure 1). FIB-4 incorporates routinely available clinical data and can be automated within electronic health records, enabling efficient risk stratification. Low-risk patients with FIB-4 values below 1.3 warrant periodic monitoring.1,3,5 Intermediate-risk patients with values between 1.3 and 2.67 should undergo VCTE or ELF testing.1,3,5 VCTE should be interpreted using established thresholds: liver stiffness values <8 kPa indicate low risk for advanced fibrosis, 8–12 kPa suggest intermediate risk requiring further evaluation with MRE or hepatology referral, and >12 kPa indicate advanced fibrosis or cirrhosis and warrant hepatology referral and surveillance.1 High-risk individuals with FIB-4 values above 2.67 should be referred directly to hepatology.1,3,5 Diabetes-focused studies increasingly support such stratified algorithms as cost-effective strategies to improve detection of advanced fibrosis.5

The use of the FIB-4 score within this diagnostic approach requires careful interpretation. FIB-4 demonstrates a high negative predictive value (NPV ≥90%) for excluding advanced fibrosis, supporting its role as an effective first-line screening tool.1,5 However, its specificity is reduced in intermediate-risk categories (approximately 71% at the <1.3 cutoff), necessitating confirmatory testing.1,5 In adults aged 65 years or older, age-related score inflation may further compromise accuracy and increase false-positive results. Sequential diagnostic algorithms that integrate FIB-4 with elastography substantially improve diagnostic performance, achieving posterior probabilities of cirrhosis ≥89% and mitigating the limitations of FIB-4 when used in isolation.1,5
Routine integration of noninvasive fibrosis assessment into GLP-1 RA prescribing pathways may fundamentally shift MASLD care. Early identification of advanced fibrosis enables timely intervention, reduces decompensated presentations, and optimizes the utilization of subspecialty resources. This approach reframes GLP-1 therapy as one component of comprehensive metabolic and hepatic risk management rather than a surrogate for liver protection. In this case, noninvasive fibrosis assessment should have been performed before initiating GLP-1 RA. Given his elevated FIB-4 score, the patient should have undergone confirmatory testing with VCTE or ELF and been referred to hepatology. Earlier recognition of advanced fibrosis would have facilitated surveillance, therapeutic optimization, and transplant evaluation, potentially preventing clinical decompensation.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding author
Eder Luna-Ceron, M.D, M.Sc.
Department of Internal Medicine,
Texas Tech University Health Sciences Center,
El Paso, Texas, United States, 79905
Email: elunacer@ttuhsc.edu