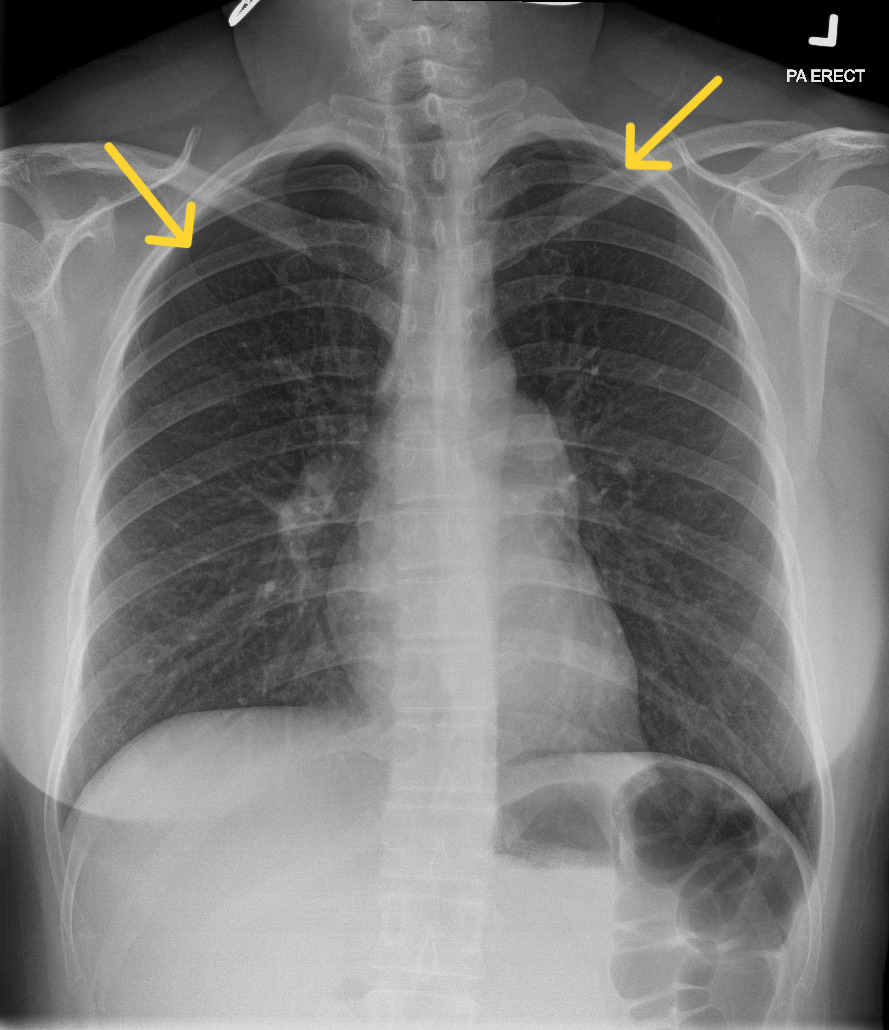
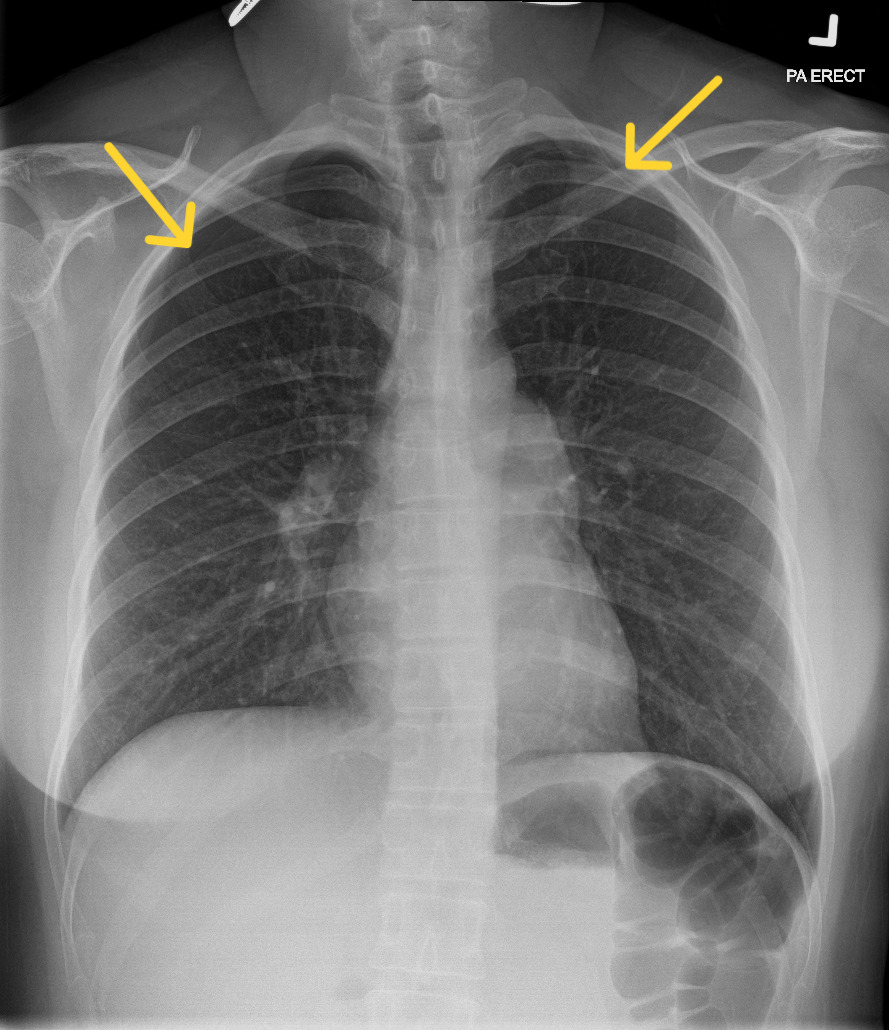
A 39-year-old Chinese woman presented to the Emergency Department with acute chest tightness and shortness of breath, which started after she completed an acupuncture session for her long-standing neck pain. Specifically, she underwent needle insertion at several acupoints, including GB21 (Jianjing), located at the crest of the trapezius muscle near the apices of the lungs. She had been well prior to acupuncture. On arrival, she was hemodynamically stable, afebrile, with normal oxygen saturations on room air. On examination, there was reduced air entry over the bilateral lung apices, but the rest of the systemic examination was unremarkable. A chest radiograph showed bilateral apical pneumothoraces, measuring up to 1.6cm on the right and 0.6cm on the left (apex-to-cupola distance) (Figure 1). Given her stable clinical status and absence of hemodynamic compromise, a trial of conservative management with supplemental oxygen therapy was given with close observation. Serial chest radiographs demonstrated resolution of the pneumothoraces, and she was discharged without the need for chest tube insertion.
Acupuncture is a cornerstone of traditional Chinese medicine (TCM), which has been used for pain relief, stress relief, and the management of various chronic health conditions. In recent years, it has been increasingly incorporated into Western medicine as a therapeutic modality for the control of acute and chronic pain.1 Though generally safe when performed by trained practitioners, adverse events may occur, usually involving minor complications such as mild bleeding, needling site pain, or paradoxical aggravation of underlying symptoms.2 Very rarely, it can lead to life-threatening complications such as pneumothorax, cardiac tamponade, nerve injury, major vessel injury/pseudoaneurysm, and migration of broken acupuncture needles.3 Out of the serious adverse iatrogenic events reported, pneumothorax is the most common, with an estimated prevalence of 0.8-2 per 100,000 cases.4
Specifically, acupuncture-associated pneumothorax typically occurs when thoracic acupoints are selected.5 Acupuncture is often performed at these areas for patients who experience shoulder and neck pains; however, its close anatomical relationship to the lung apex (10-29 mm in males, 12-20 mm in females, depending on body build) renders it a high-risk point.5 Specifically, among the thoracic acupoints, Jianjing (GB21) is a particularly high-risk acupoint for pneumothorax, with a previous study showing that 30% of acupuncture-associated pneumothorax cases were associated with the use of this acupoint.6 In lean build patients or specific postures (sitting), the risk of iatrogenic pneumothorax, especially if the procedures misjudge the insertion depth, is accentuated.5 In Western societies, deep dry needling, a practice often seen as a corollary to Eastern acupuncture, which is performed by osteopathic practitioners and physical therapists for relief of musculoskeletal symptoms, has also reportedly led to rare cases of iatrogenic pneumothorax.7
Formal accreditation training is essential for practitioners of complementary and alternative medicine, such as acupuncturists and physical therapists. For safe thoracic acupuncture, traditional teaching recommends that practitioners ensure a shallow insertional depth of 12mm at GB21, adopt the posterior oblique insertion technique of 0.5-1cun (1 cun ~ 3.33 cm) with lifting of trapezius and front-to-back needling, and opt for prone rather than seated positioning of the patient.5 Recently, ultrasound-guided thoracic acupuncture has also been recommended, which is the standard practice for other thoracic procedures like thoracocentesis.8 All patients who are undergoing thoracic acupunctures should be properly counselled on the potential risk of iatrogenic pneumothorax. They should also be provided with return advice in the event of breathlessness and chest pains, in which case early recognition and prompt imaging are essential to avoid potentially life-threatening complications of untreated pneumothorax.
Disclosures/Conflicts of Interest
None
Corresponding author
Dr Wilson GW Goh
Division of Infectious Disease
Department of Medicine
National University Hospital, Singapore
5 Lower Kent Ridge Road Singapore 119074
Email: wilson.goh@mohh.com.sg