Background
Crohn’s disease is a chronic inflammatory gastrointestinal disorder that commonly leads to strictures in young adults and is diagnosed using characteristic clinical, radiologic, endoscopic, and histologic features.1 However, infectious, ischemic, and neoplastic processes may closely mimic Crohn’s disease and complicate diagnosis.2 Among these, diffuse-type gastric adenocarcinoma is particularly deceptive because of its submucosal growth pattern and preserved mucosal integrity, which often result in false-negative endoscopic biopsies.3 Signet-ring cell carcinoma, a histologic subtype of diffuse gastric cancer, is aggressive and frequently presents with peritoneal dissemination at diagnosis.4,5 Here, we report a case of metastatic gastric signet-ring cell carcinoma mimicking Crohn’s disease, highlighting the importance of maintaining diagnostic vigilance when atypical features are present.
Case Report
A 39-year-old woman with a history of gastritis and hiatal hernia presented to the emergency department with several months of cramping abdominal pain, watery diarrhea occurring four times daily, bilious emesis, and progressive intolerance to solid foods. She also reported an unintentional 34-pound weight loss over the preceding 6 months. Several weeks before presentation, she had been hospitalized elsewhere for presumed infectious colitis and was discharged on oral ciprofloxacin and metronidazole. She denied hematochezia, fever, and any family history of inflammatory bowel disease.
On presentation, her temperature was 98.5°F, blood pressure 105/71 mmHg, heart rate 86 beats/min, respiratory rate 18 breaths/min, and oxygen saturation 98% on room air. She appeared thin and chronically ill. Abdominal examination was notable for diffuse tenderness and hyperactive bowel sounds, without rebound, guarding, or other peritoneal signs. There were no clinical stigmata of portal hypertension, including ascites on examination, splenomegaly, palmar erythema, or spider angiomata. Initial laboratory evaluation demonstrated microcytic anemia, with hemoglobin 9.2 g/dL (reference range, 12-16 g/dL), hematocrit 29.6% (36-46%), and mean corpuscular volume 70 fL (80-100 fL). The white blood cell count was 7.3 × 10³/μL (4-11 × 10³/μL), and the platelet count was 374 × 10³/μL (150-400 × 10³/μL). Iron studies were notable for ferritin 8.3 ng/mL (15-150 ng/mL). C-reactive protein was 3.3 mg/L (<5 mg/L). The comprehensive metabolic panel showed sodium 137 mmol/L (136-145 mmol/L), potassium 3.3 mmol/L (3.5-5.1 mmol/L), creatinine 0.6 mg/dL (0.6-1.2 mg/dL), and albumin 4.3 g/dL. Liver panel was within normal limits, including alanine aminotransferase 9 U/L (7-56 U/L), aspartate aminotransferase 13 U/L (10-40 U/L), alkaline phosphatase 70 U/L (45-115 U/L), and total bilirubin 0.5 mg/dL (0.1-1.2 mg/dL).
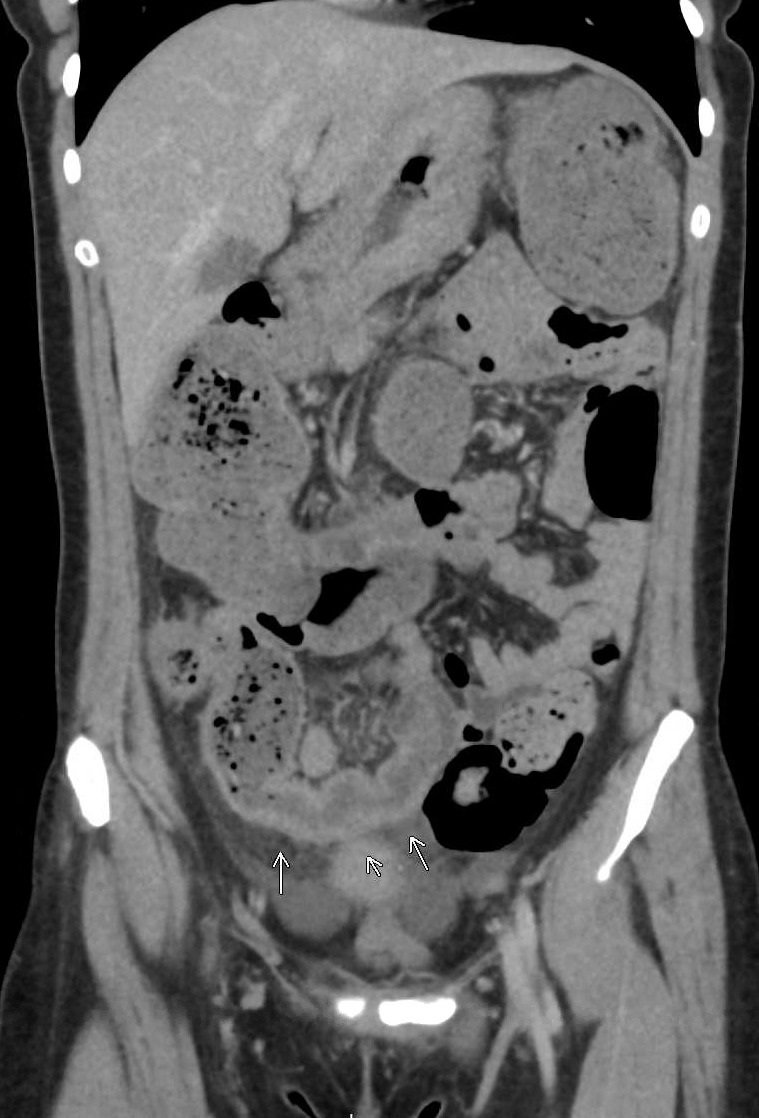
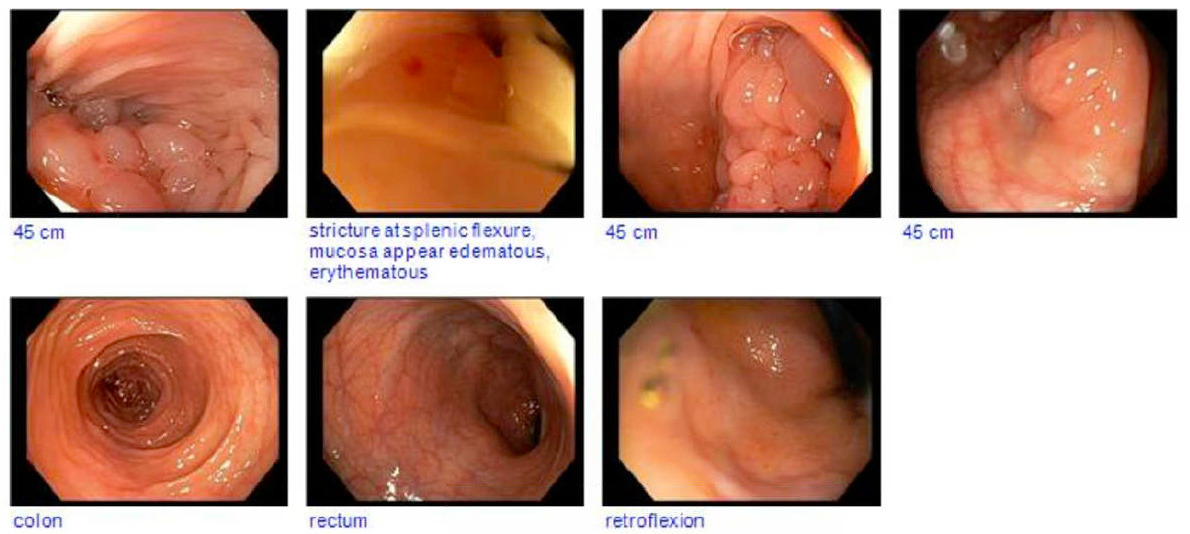
On hospital day 1, contrast-enhanced computed tomography of the abdomen and pelvis demonstrated circumferential wall thickening with surrounding fat stranding extending from the cecum to the mid-ascending colon, along with an abrupt transition at the splenic flexure and upstream colonic dilation (Figure 1A). Given concern for inflammatory bowel disease, bidirectional endoscopy was performed on hospital day 5. Esophagogastroduodenoscopy revealed obliterated gastric folds and diffusely congested mucosa, with limited retroflexion because of marked edema. Multiple large-cap cold forceps biopsies were obtained from the gastric body and antrum. Histopathologic examination demonstrated chronic inactive gastritis without evidence of Helicobacter pylori infection. Endoscopic ultrasound was not performed, and no submucosal sampling was obtained. Colonoscopy showed normal-appearing mucosa to 45 cm from the anal verge; beyond this point, the lumen was nearly obliterated by edematous, congested tissue, resulting in a nontraversable stricture (Figure 1B). Biopsies from the stricture demonstrated only nonspecific reactive changes.


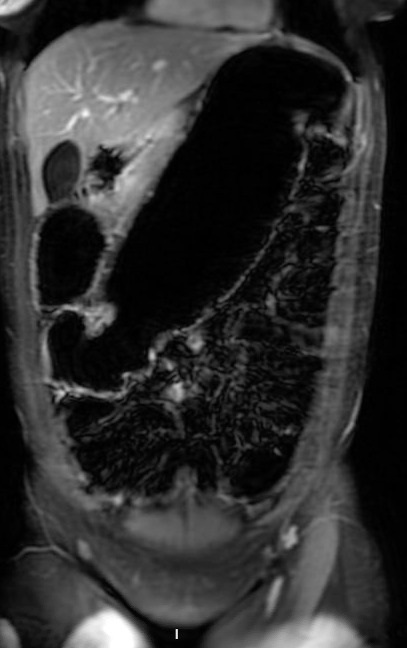
Magnetic resonance enterography on hospital day 7 confirmed mural thickening and luminal narrowing of the descending colon with upstream distension, findings suggestive of a chronic stricture (Figure 1C). Moderate-volume pelvic ascites was also present, although there were no imaging features of portal hypertension. An extensive infectious and inflammatory evaluation, including stool cultures, ova and parasite examination, celiac serologies, tuberculosis testing, and serologic testing for Entamoeba histolytica, was unrevealing. Although ascites was present, no safe fluid pocket was available for diagnostic paracentesis. Because of progressive obstructive symptoms, worsening colonic dilation, and persistent diagnostic uncertainty despite extensive noninvasive evaluation, laparoscopic-assisted subtotal colectomy was performed on hospital day 8. Empiric immunosuppressive therapy for Crohn’s disease was deferred throughout the evaluation because of the absence of classic endoscopic features of inflammatory bowel disease and concern for an alternative diagnosis. Intraoperatively, multiple colonic strictures, adhesions involving the pancreas and spleen, mesenteric lymphadenopathy, and diffuse gastric wall thickening were identified.

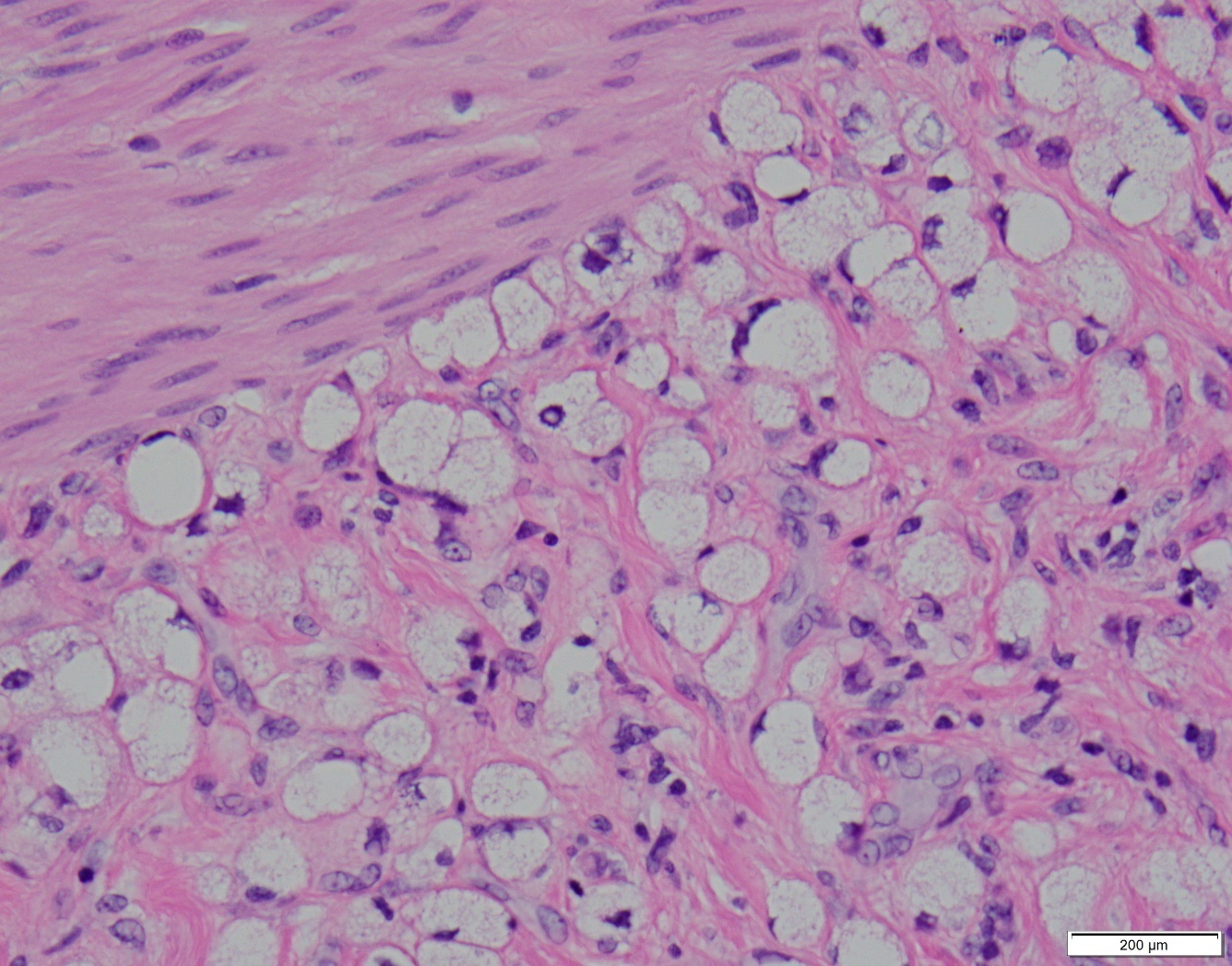
Gross examination of the resected specimen demonstrated long-segment mural thickening and induration. Histopathologic analysis revealed diffuse infiltration by signet-ring cells involving the submucosa and muscularis of the colon, appendix, and terminal ileum, consistent with metastatic gastric adenocarcinoma (Figure 1D). Immunohistochemistry supported a gastric primary. Four of 31 lymph nodes were positive for metastatic disease. Postoperative positron emission tomography-computed tomography demonstrated fluorodeoxyglucose-avid lesions in the gastric body and left adnexa, as well as left-sided hydroureteronephrosis. The patient was subsequently referred to medical oncology and initiated on palliative chemotherapy with 5-fluorouracil, leucovorin, and oxaliplatin.
_of_resected_colon_demonstrating_infiltration_of_signet-r.jpeg)
Discussion
Colonic strictures arise from a broad range of etiologies, among which inflammatory bowel disease and malignancy represent two critical diagnoses that require careful distinction. In Crohn’s disease, chronic transmural inflammation leads to fibrosis and stricture formation, often accompanied by characteristic features such as skip lesions, mucosal ulceration, cobblestoning, and fistulizing disease.1,2 In contrast, signet-ring cell carcinoma presents a distinct pathophysiologic challenge. This malignancy is characterized by diffuse infiltration of individual tumor cells or small clusters within the submucosa and muscularis, often with preservation of the mucosal surface.3,4 This growth pattern results in mural thickening and luminal narrowing that can radiographically and endoscopically mimic inflammatory strictures.
In this case, the patient’s age, chronic diarrhea, and imaging findings initially supported a diagnosis of Crohn’s disease. However, several features were atypical. C-reactive protein was within normal limits, ferritin was low at 8.3 ng/mL in keeping with iron-deficiency anemia rather than anemia of chronic disease, and platelet count, although at the upper end of normal (374 × 10³/µL), did not demonstrate frank reactive thrombocytosis. The presence of moderate-volume pelvic ascites without radiographic evidence of portal hypertension is uncommon in inflammatory bowel disease. In our patient, the ascites was first recognized on MR enterography, but the lack of a safe, image-guided window for diagnostic paracentesis limited further characterization before surgery. Endoscopy failed to demonstrate hallmark features of Crohn’s disease, including aphthous or serpiginous ulcers, cobblestoning, or friable mucosa. Instead, the patient exhibited severe, abrupt luminal narrowing with edematous but intact mucosa, suggestive of a submucosal infiltrative process. Additionally, profound weight loss and only mildly elevated inflammatory markers were discordant with the degree of structural disease observed.1,2
Signet-ring cell carcinoma accounts for approximately 10-20% of gastric adenocarcinomas and is associated with particularly poor prognosis.4 This histologic subtype is defined by the presence of intracellular mucin accumulation that displaces the nucleus to the cell periphery, creating the characteristic signet-ring appearance. The diffuse-type growth pattern, as described by Lauren in 1965, is characterized by infiltration of individual tumor cells or small clusters throughout the gastric wall with minimal glandular formation.3 Because tumor cells preferentially spread within the submucosa, superficial endoscopic biopsies may be non-diagnostic, with false-negative rates of 30–40% reported.4,5 At presentation, signet-ring cell carcinoma commonly demonstrates peritoneal dissemination, with peritoneal carcinomatosis occurring in 10-20% of cases.4,5 The phenomenon of colonic metastases from gastric primary malignancies is well-documented but relatively uncommon. When gastric cancer metastasizes to the colon, it typically involves serosal implantation or direct extension rather than hematogenous spread. The resulting colonic involvement can create strictures that may be mistaken for primary colonic pathology or inflammatory conditions.6 Metastatic gastric signet-ring cell carcinoma carries a poor prognosis, with many patients presenting with peritoneal dissemination and limited survival despite systemic chemotherapy, underscoring the importance of early recognition when evaluating atypical stricturing disease.4,5
Management of malignant strictures secondary to signet-ring cell carcinoma requires a multidisciplinary approach involving gastroenterology, radiology, surgery, pathology, and medical oncology. When endoscopic biopsies are non-diagnostic, but clinical suspicion for malignancy remains high, alternative diagnostic strategies should be pursued. These include endoscopic ultrasound with fine-needle aspiration to sample deeper layers, repeat endoscopy with jumbo or deep biopsies, or surgical exploration when obstruction or progressive symptoms are present.7–9 In this case, endoscopic ultrasound was not performed before surgery; however, EUS-guided sampling of the gastric wall or pericolonic tissue might have facilitated earlier tissue diagnosis in the setting of nondiagnostic mucosal biopsies. In our case, subtotal colectomy served both diagnostic and therapeutic purposes, relieving obstruction while providing definitive histopathologic diagnosis.
Systemic chemotherapy remains the mainstay of treatment for metastatic signet-ring cell carcinoma, although response rates are generally lower than for other gastric cancer subtypes. Fluoropyrimidine-based regimens are commonly employed, with targeted or immunotherapeutic options reserved for select molecular profiles.5 Palliative interventions, including surgical bypass, ostomy creation, or endoscopic stenting, play an essential role in symptom management for patients with malignant bowel obstruction.10
Conclusion
This case highlights the importance of maintaining a broad differential diagnosis when evaluating patients with suspected inflammatory bowel disease, particularly when atypical features are present. Unexplained ascites, severe stricturing with preserved mucosa, disproportionate weight loss, or discordance between clinical severity and inflammatory markers should prompt reconsideration of the diagnosis. The limitations of superficial endoscopic biopsies must be recognized when evaluating submucosal processes such as diffuse-type gastric adenocarcinoma. When clinical suspicion persists despite negative biopsies, deeper tissue sampling or surgical intervention is warranted. Finally, multidisciplinary collaboration is essential for timely diagnosis and management. Young age should not be falsely reassuring, as aggressive gastric malignancies can present early and masquerade as inflammatory disease. Early recognition of malignant mimics is critical to avoiding diagnostic delay and optimizing patient care.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding Author
Samantha Zullow, MD
Beth Israel Deaconess Medical Center
330 Brookline Ave, Boston, MA 02215
Email: szullow@bidmc.harvard.edu