Background
Pickering syndrome is an uncommon but clinically significant entity characterized by recurrent episodes of severe hypertension and flash pulmonary edema in the setting of renovascular disease. It is classically associated with bilateral renal artery stenosis (RAS) or unilateral RAS in a solitary functioning kidney, where reductions in renal perfusion trigger activation of the renin–angiotensin–aldosterone system (RAAS) and lead to abrupt cardiopulmonary decompensation.1 Although initially described in older adults with diffuse atherosclerotic disease, Pickering syndrome has also been reported in younger patients and in association with non-atherosclerotic causes of renovascular hypertension.2 In younger individuals, renovascular disease may arise from conditions such as fibromuscular dysplasia, vasculitis (including Takayasu arteritis), neurofibromatosis-associated vasculopathy, congenital renal artery anomalies, or focal segmental arterial abnormalities. Recognition of these non-atherosclerotic etiologies is particularly important when evaluating severe or early-onset hypertension.
We present a young woman with recurrent hypertensive emergencies and flash pulmonary edema in whom intrarenal Doppler ultrasonography demonstrated a probable focal abnormality confined to an upper-pole segmental renal artery. This case highlights a probable focal intrarenal renovascular mechanism producing a clinical presentation suggestive of Pickering physiology.
Case Presentation
A 34-year-old woman had a family history notable for early-onset hypertension, congestive heart failure, and chronic kidney disease (CKD) in her father before the age of 50, as well as CKD in a paternal uncle. She had a prior 15–pack-year smoking history and reported prior marijuana use and heavy alcohol consumption during adolescence, with cessation of tobacco and alcohol use by 2020. In June 2024, she presented with a hypertensive emergency, with a blood pressure of 254/162 mmHg, accompanied by severe headache, visual blurring, and retinal hemorrhage. Laboratory evaluation demonstrated acute kidney injury (serum creatinine 1.69 mg/dL) and marked hypokalemia (serum potassium 2.2 mmol/L), with an elevated NT-proBNP of 6,174 pg/mL. The plasma aldosterone–to–plasma renin ratio was within normal limits. Transthoracic echocardiography revealed preserved left ventricular ejection fraction (LVEF) with concentric left ventricular hypertrophy and grade I diastolic dysfunction. She improved with intravenous nicardipine and was discharged on two oral antihypertensives.
Three months later, in September 2024, she re-presented with shortness of breath, melena, abdominal discomfort, and uncontrolled hypertension (177/111 mmHg). Laboratory evaluation revealed severe acute kidney injury (serum creatinine 8.65 mg/dL), anemia (hemoglobin 6.9 g/dL), thrombocytopenia, schistocytes on peripheral smear, and markedly elevated NT-proBNP levels (>35,000 pg/mL). Chest radiography demonstrated new pulmonary edema. ADAMTS13 activity was within normal limits, and hematology attributed the microangiopathic hemolytic anemia to uncontrolled hypertension rather than thrombotic thrombocytopenic purpura. She was again hospitalized in November 2024 with a blood pressure of 233/136 mmHg. Laboratory evaluation demonstrated advanced renal dysfunction (creatinine 9.63 mg/dL, BUN 80 mg/dL) and an elevated NT-proBNP of 11,319 pg/mL. She required intravenous nitroglycerin followed by nicardipine infusion, after which she was transitioned to three oral antihypertensives.
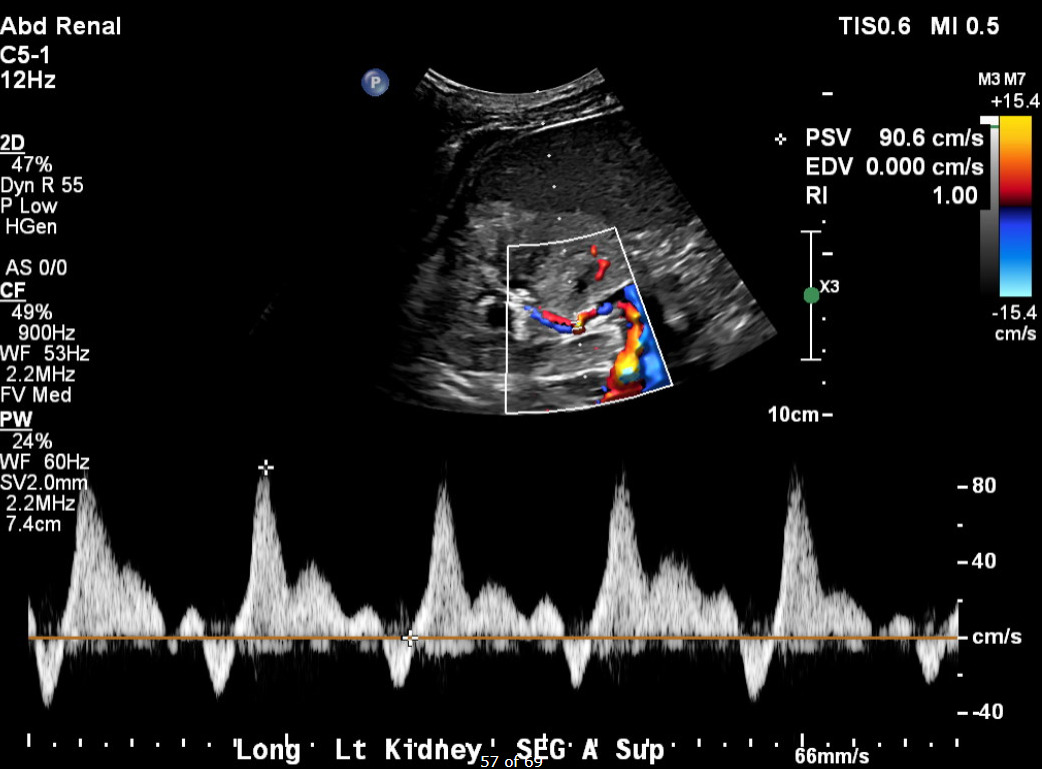
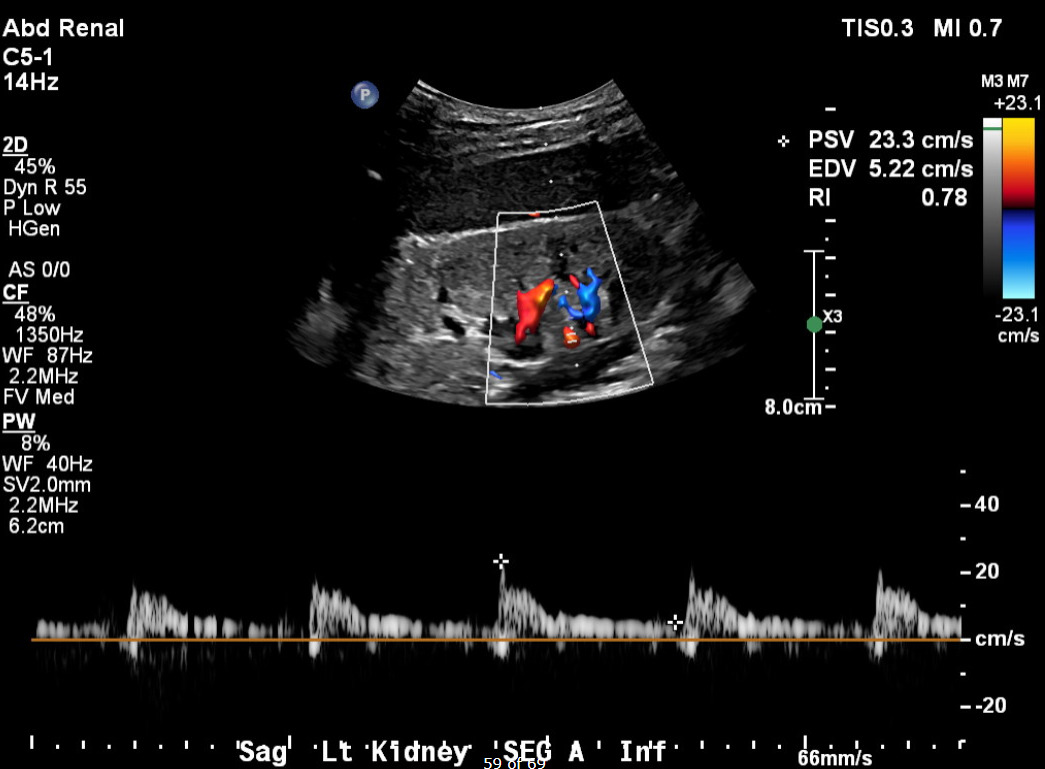
Her current presentation was characterized by a one-week history of worsening dyspnea, orthopnea, and paroxysmal nocturnal dyspnea. On arrival, her blood pressure was 257/169 mmHg, with tachypnea and bilateral inspiratory crackles on examination. Initial laboratory studies (Table 1) demonstrated serum creatinine 5.36 mg/dL, BUN 74 mg/dL, hemoglobin 8.2 g/dL, NT-proBNP >35,000 pg/mL, and high-sensitivity troponin T 93 ng/L, consistent with demand ischemia in the setting of hypertensive emergency. Urinalysis revealed 3+ proteinuria. Chest radiography demonstrated bilateral interstitial and alveolar opacities consistent with pulmonary vascular congestion. A transthoracic echocardiogram obtained during this admission demonstrated preserved LVEF (56–60%), severe concentric left ventricular hypertrophy, and grade I diastolic dysfunction. Renal duplex ultrasonography demonstrated bilaterally echogenic kidneys consistent with medical renal disease. Doppler interrogation of a segmental branch supplying the upper pole of the left kidney demonstrated elevated peak systolic velocity (~90.6 cm/s), absent end-diastolic flow (end-diastolic velocity 0.0 cm/s), and a markedly elevated resistive index (RI = 1.0) (Figure 1), findings which may suggest severe intrarenal hemodynamic compromise and a probable functionally significant focal upper-pole segmental renal artery stenosis. Flow velocities in the main renal arteries and other segmental branches were within normal limits (Figure 2). Computed tomographic angiography was not performed due to advanced renal dysfunction. Magnetic resonance angiography was also considered; however, it was not pursued during this hospitalization because additional imaging was unlikely to alter immediate management, particularly in the setting of advanced chronic kidney disease and the patient’s preference to avoid renal replacement therapy.


In this patient with recurrent hypertensive emergencies, flash pulmonary edema, and progressive renal dysfunction, several diagnoses were considered. Primary hypertension was initially suspected; however, the severity, recurrence, and associated pulmonary edema were disproportionate to primary hypertension alone. Cardiogenic pulmonary edema due to systolic heart failure was excluded based on preserved left ventricular systolic function on serial echocardiography. Thrombotic microangiopathy was considered during episodes of anemia, thrombocytopenia, and schistocytosis, but normal ADAMTS13 activity supported secondary microangiopathic hemolytic anemia related to severe hypertension. Primary hyperaldosteronism was considered given initial hypokalemia, but a normal aldosterone–to–renin ratio made this diagnosis unlikely. Renal parenchymal disease was supported by bilaterally echogenic kidneys and chronic kidney disease, but did not fully explain the episodic flash pulmonary edema alone. In contrast, focal abnormal intrarenal Doppler findings in the setting of reduced renal functional reserve supported renovascular hypertension with Pickering physiology.
She was admitted to the intensive care unit for a hypertensive emergency complicated by acute pulmonary edema. Her respiratory status improved with high-dose intravenous diuretics and control of blood pressure with nicardipine infusion, followed by transition to oral hydralazine, carvedilol, isosorbide dinitrate, and amlodipine. She was discharged with close outpatient follow-up with nephrology. Renin–angiotensin–aldosterone system blockade with an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker was considered; however, initiation was deferred given the patient’s advanced chronic kidney disease and recurrent episodes of acute kidney injury, with concern for further deterioration in renal function.
Discussion
This case illustrates an atypical renovascular presentation of Pickering physiology in a young patient with focal intrarenal vascular disease. Unlike the classic description involving bilateral renal artery stenosis or stenosis in a solitary functioning kidney, our patient demonstrated recurrent hypertensive emergencies and flash pulmonary edema in the setting of a probable focal segmental renovascular abnormality. The combination of preserved left ventricular systolic function, markedly elevated natriuretic peptide levels, and repeated episodes of pulmonary edema suggested a hemodynamic process driven primarily by renovascular hypertension rather than intrinsic cardiac dysfunction. These findings highlight how probable localized intrarenal vascular compromise, particularly in the setting of reduced renal functional reserve, may produce systemic hemodynamic consequences similar to those traditionally attributed to more extensive renovascular disease. Unlike other reported cases, which involve older patients with diffuse atherosclerotic disease, this patient experienced recurrent hypertensive emergencies and flash pulmonary edema beginning in early adulthood. Similar to previously described cases, she demonstrated preserved left ventricular systolic function with concentric hypertrophy and diastolic dysfunction, a cardiac substrate known to predispose patients to abrupt pulmonary congestion in the setting of acute afterload elevation.2,3
Several reports have demonstrated that unilateral renal artery stenosis may precipitate flash pulmonary edema when renal functional reserve is reduced, including cases involving contralateral kidney atrophy or solitary kidneys.4–6 These observations support the concept that loss of effective renal mass, rather than anatomic bilaterality alone, may reproduce the physiologic consequences traditionally attributed to bilateral disease. In our patient, advanced chronic kidney disease likely amplified the hemodynamic impact of the focal segmental lesion, allowing a localized vascular abnormality to produce recurrent systemic decompensation. Building on this, the case further emphasizes the importance of thorough renovascular evaluation, even when abnormalities appear subtle. Segmental or branch-level renal artery stenosis can be missed when diagnostic evaluation is limited to the main renal arteries, as Doppler criteria validated for main artery disease may not reliably identify focal branch involvement⁷. Seoung et al. showed that systematically comparing intrarenal Doppler waveforms across multiple renal segments (upper, mid, and lower poles), and noting significant regional hemodynamic differences, can suggest the presence of a hemodynamically important focal lesion.7 In this case, duplex ultrasonography demonstrated abnormal renal arterial hemodynamics confined to an upper-pole segmental branch (Figure 1), while waveforms in other intrarenal segments were preserved (Figure 2). This regional disparity may support the presence of focal segmental renovascular disease. This pattern has been reported as a cause of renovascular hypertension but remains susceptible to under recognition.7
Although computed tomographic angiography could not be performed because of advanced renal dysfunction, duplex Doppler ultrasonography remains a validated noninvasive tool for renovascular assessment. Intrarenal Doppler abnormalities, including absent or reversed end-diastolic flow and elevated resistive indices, have been described as surrogate indicators of hemodynamically significant renovascular disease when main renal artery velocities are normal; however, these findings represent indirect evidence and must be interpreted in conjunction with clinical features and renal functional reserve.8
The management of Pickering syndrome remains individualized, particularly in patients with advanced chronic kidney disease. Multiple reports have demonstrated improved blood pressure control and reduced recurrent pulmonary edema following renal artery revascularization in selected patients.3,4 However, therapeutic decisions must take into account procedural risks, renal reserve, and patient preferences. In this case, interventional options were limited by advanced chronic kidney disease, the absence of angiographic confirmation, and the patient’s refusal of renal replacement therapy. As a result, no interventional radiology recommendation for revascularization was made. Management, therefore, focused on aggressive medical control of blood pressure, volume management, and close outpatient follow-up. Nonetheless, identification of a likely underlying renovascular mechanism provided important insight into her recurrent presentations and informed prognostic counseling, allowing care to emphasize medical optimization and patient-centered counseling.
Conclusion
This case expands the recognized clinical spectrum of Pickering syndrome by demonstrating that focal segmental renovascular disease may precipitate recurrent hypertensive emergencies and flash pulmonary edema in a patient with reduced renal reserve. Recognition of atypical renovascular patterns may prevent diagnostic delay and reduce recurrent cardiopulmonary decompensation.
Disclosures/Conflicts of Interest
The authors declare that they have no conflicts of interest.
Corresponding author
David K. A. Donkor, MD
Department of Internal Medicine
Wellstar Spalding Regional Hospital
601 South 8th Street, Griffin, GA 30224, USA
Email: asedakd8@gmail.com