Background
Delirium is an acute state of confusion that arises in up to a quarter of hospitalized older adults and up to 80% of intensive-care patients.1,2 It is associated with increased patient morbidity and mortality, and contributes to an estimated annual national cost of $32.9 billion.1,3,4 Despite its high prevalence, delirium is often underdiagnosed and sub-optimally managed in clinical practice.5
Effective delirium management is multifactorial and centers on addressing modifiable risk factors, preserving cognition and orientation, and optimizing patients’ vision, hearing, sleep, and mobility.6,7 These supportive or de-escalating strategies have been proven to reduce complications such as falls, prolonged hospitalization, and long-term cognitive decline.7 However, they are commonly underutilized in favor of restraints and pharmacological intervention due to time pressure and competing clinical demands, among other factors.
To optimize delirium management at our institution, we implemented a clinical decision support system (CDSS) within our Epic (Verona, Wisconsin, USA) electronic medical record (EMR). Our institution previously integrated routine universal delirium screening into nursing workflow, using the 4 A’s Test (4AT, assessing alertness, orientation, attention, acuteness, and fluctuation of change), enabling point-of-care alerts to physicians regarding a patient’s delirium risk.8 We introduced an Our Practice Advisory (OPA) and order set, triggered by a positive 4AT delirium risk score, designed to encourage high-value interventions and discourage unnecessary medication use or other low-value procedures. This study aims to evaluate the utilization of this intervention and its impact on encouraging adherence to evidence-based delirium management practices at our institution.
Methods
Study Design and Setting
This quasi-experimental pre-post study was conducted at two hospitals within an urban academic medical center using the Epic EMR system. Our intervention was implemented as a quality improvement initiative to optimize delirium management for hospitalized general medicine patients.
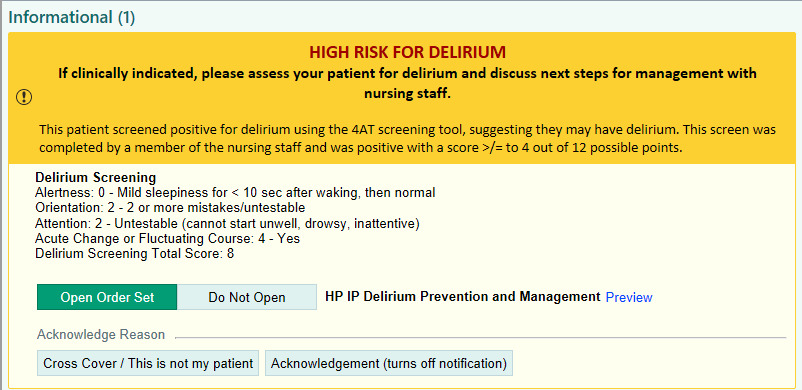
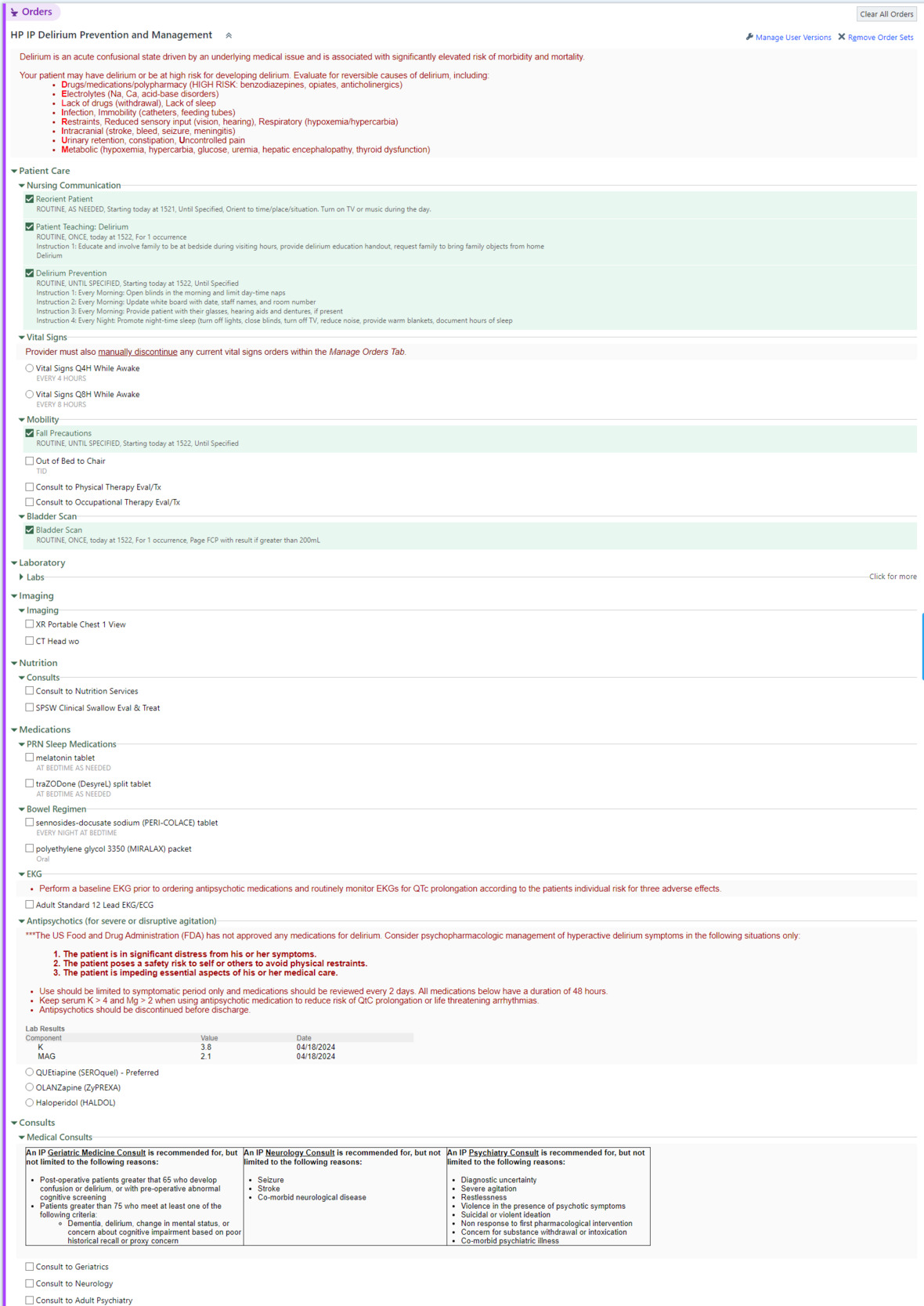
The OPA (Figure 1), triggered once daily by a positive 4AT delirium screen (score ≥4), alerts hospitalists to a patient’s delirium risk and provides one-click access to the order set or the option to deactivate the alert. The order set (Figure 2) was informed by a literature review and feedback from a multidisciplinary Delirium Taskforce. It was designed to influence clinician behavior at the point of ordering by surfacing delirium risk and emphasizing high-value management strategies. It highlights supportive interventions such as reorientation and sleep hygiene, while discouraging antipsychotics and benzodiazepines by default collapsing the antipsychotic/benzodiazepine section. Mechanical restraint orders were intentionally excluded from the order set; orders for restraints remained available elsewhere in the EMR and required a separate order search. The OPA was programmed to activate once per patient per day to avoid alert fatigue. Prior to the intervention launch, targeted training sessions were conducted for hospitalists on OPA activation and order set utilization. The intervention was implemented at Hospital 1 in January 2024 and Hospital 2 in June 2024.
_triggered_by_positive_delirium_screen.png)

Data Collection and Analysis
Data were collected over a 6-week pre-intervention period and a 6-month post-intervention period at both hospitals. Outcomes included utilization of antipsychotics and/or benzodiazepines, mechanical restraints, standing bowel regimen orders, and provider engagement with the OPA. For medication use, we recorded whether patients were prescribed any antipsychotics and/or benzodiazepines following a positive 4AT; medication dosage, indication, or continuation from prior to admission were not evaluated. Encounters in which the OPA did not trigger appropriately were excluded from analysis. Descriptive statistics were used to summarize patient characteristics. Statistical analysis of pre- versus post-intervention differences was performed using t-tests. Given the intervention’s quality-improvement focus, analyses focused on changes in utilization patterns rather than causal inference. Statistical significance was determined with p<0.05.
Results
There were 359 patients in the pre-intervention period and 521 in the post-intervention period. Groups had similar age (77.6 vs 78.4 years) and sex distribution (44.0% vs 40.5% male). There was an imbalance in race distribution, with a greater number of Black patients post-intervention (71.0% vs 80.4%, p=0.01). The pre-intervention group had a higher peak 4AT score (6.7 vs 6.2, p=0.003).
Our intervention was associated with a significant decrease in mechanical restraint use (35.4% to 23.4%, p<0.001). There was no significant change in antipsychotic and/or benzodiazepine use (25.6% vs 25.0%, p=0.82). Standing bowel regimen orders decreased (from 56.0% to 46.7%, p=0.014), rather than increasing as intended. Of 521 OPA activations, 40.7% resulted in new orders placed, 35.7% involved providers opening the order set without placing new orders, and 23.6% of alerts were disregarded (Table 1).
Discussion
In this quasi-experimental study, implementation of an EMR-embedded clinical decision support tool was associated with a decline in mechanical restraint use among hospitalized patients at risk for delirium. This finding suggests the success of the order set in influencing provider behavior to align with evidence-based delirium management practices.9
The observed reduction in mechanical restraint use is likely attributable to the behavioral design of the order set, which placed supportive, non-pharmacologic care options at the forefront while omitting the option to order restraints entirely. Although it was possible to order restraints elsewhere in the EMR, exclusion from the order set served as a point-of-care reminder for clinicians to prioritize non-restrictive strategies and to reconsider initiating restraints or discontinuing them when no longer necessary. Prior studies of clinical decision support tools have demonstrated that incorporating behavioral design, such as altered defaults or restricted access to lower-value choices, can meaningfully shift clinician behavior without increasing cognitive burden.10 Our study demonstrates the application of these principles to delirium management.
In contrast, antipsychotic and/or benzodiazepine use remained unchanged. This may reflect entrenched prescribing patterns, continuation of medications from prior to admission, or scenarios in which pharmacologic management was deemed clinically necessary. We measured medication initiation as a binary outcome and did not distinguish new initiations for delirium from continuation of chronic regimens or use for other indications. This may have masked a true effect from the intervention on prescribing practices specifically for delirium management. Antipsychotics and benzodiazepines were not entirely removed from the ordering pathway, as restraint use was, which may in part explain the observed lack of effect. Standing bowel regimen orders decreased rather than increased as intended. Potential explanations for this include order placement outside the delirium order set (e.g., regimens ordered via admission or nursing protocols), greater provider selectivity in ordering standing regimens due to differences in patient mix or clinical context between periods, shifts in prescribing norms unrelated to the intervention, and alert fatigue or competing priorities within the order set. Future iterations could improve visibility by placing the option for bowel regimen orders higher in the order set.
Differences in patient characteristics between the pre- and post-intervention periods may have contributed to the study outcomes, a major limitation of the pre-post design. The pre-intervention group had a higher peak 4AT score, indicating greater delirium severity, which could have facilitated decreases in mechanical restraint utilization. Notably, restraint use decreased in the post-intervention group despite a higher proportion of Black patients, a population found to experience higher use of mechanical restraints compared to other racial groups.11 However, the significant variation in racial demographics between the pre- and post-groups limits our ability to attribute the decrease of restraint use solely to the intervention. Future work should stratify analyses by delirium severity and patient demographics.
Over 40% of OPA activations resulted in order set utilization, demonstrating robust engagement that compares favorably to prior EMR-based interventions.12,13 Possible reasons for this level of engagement include the targeted training sessions led with hospitalists and the concise design of the OPA (Figure 1), as well as limitations placed on alert frequency to minimize alert fatigue. While CDSS tools can improve care, their value depends greatly on provider adherence.14 Alert fatigue is a major challenge, with prior studies reporting 46%-96% of alerts being overridden.15 Our mitigation efforts included carefully selecting criteria for OPA activation and limiting alerts to once daily.
This study has several limitations. This intervention was conducted at two hospitals within a single academic health system, which limits the generalizability of the findings. As previously mentioned, the lack of a contemporaneous control group in the pre-post design poses risks of residual confounding, including differences in racial demographics, delirium severity, and secular trends between the pre- and post-periods. Medication initiation did not distinguish between new medications initiated during hospitalization for delirium versus medications continued from prior to admission or initiated for other indications, which limits the ability to interpret the intervention’s impact. Finally, patient-centered outcomes were not assessed. Important priorities for future work could include assessment of delirium duration, falls, hospital length of stay, discharge disposition, and mortality.
Despite the limitations, our study suggests that intentionally designed EMR-based clinical decision support tools can lead to meaningful reductions in low-value delirium management practices. Future work can prioritize iterative refinement of the OPA and order set’s design (such as through usability testing and eliciting of provider feedback), more precise evaluation of antipsychotic/benzodiazepine prescribing changes attributable to new delirium diagnoses, and assessment of patient-centered outcomes such as delirium duration, falls, length of stay, and discharge disposition.
Conclusion
Implementation of clinical decision support for delirium awareness and management was associated with a 12% absolute decrease in restraint utilization among patients at high risk for delirium during a six-month period. Notable features of the intervention included targeted alert activation following a positive delirium screen and emphasis on high-value, non-pharmacologic orders such as frequent patient re-orientation. Ongoing efforts aim to expand this clinical decision support system to surgical and subspecialty services within our institution.
Funding information
This project was supported by the Costs of Care Students and Trainees Advocating for Resource Stewardship (STARS) program, the I-CARE grant at the University of Chicago, and the HRSA Geriatrics Workforce Enhancement Program (GWEP) grant U1QHP53056.
Disclosures/conflicts of interest
The authors declare no conflicts of interest to disclose.
Corresponding author
Robin Ji
924 E. 57th Street Biological Sciences Learning Center
Chicago, IL, 60637
Email: robinji@uchicagomedicine.org