Background
Cyclic thrombocytopenia (CTP) is a very rare hematological condition, with fewer than 100 cases described in the literature.1 It is characterized by periodic and predictable fluctuations in platelet count, including episodes of severe thrombocytopenia, and is frequently confused with immune thrombocytopenia (ITP).2 It is more prevalent in females and, unlike ITP, the response to immunosuppressive therapies is usually inconsistent, while interventions such as splenectomy often fail.3
Although it is a rare disease, it presents a clinically challenging condition, particularly regarding its management, as robust evidence supporting effective therapeutic strategies is still lacking.3 Current treatment options are largely based on extrapolations from the management of immune thrombocytopenia, considering potential pathophysiological similarities between the two conditions.1,2 In this context, case reports and case series play a crucial role by providing practical insights that help inform and guide clinical decision-making.
We report a case of long-standing cyclic thrombocytopenia, initially refractory to multiple lines of therapy. The patient developed thrombosis while on eltrombopag, and subsequently showed clinical response after treatment with rituximab.
Case presentation
A 51-year-old female patient with controlled systemic arterial hypertension and grade I obesity (BMI 32.85 kg/m²) presented with a history of severe thrombocytopenia (grades III/IV) associated with mucocutaneous bleeding since 2012, initially treated as immune thrombocytopenia. During the progression of her illness, the patient developed refractory disease and received systemic corticosteroid therapy, rescue treatments with intravenous immunoglobulin (IVIG), splenectomy with early relapse within 12 months, and azathioprine for six months, none of which resulted in a sustained response.
In 2022, eltrombopag was initiated at a dose of 50 mg/day. The patient achieved higher and more sustained platelet counts, although values remained within the normal range and did not reach thrombocytosis. Despite this partial stabilization, episodes of severe thrombocytopenia persisted, accompanied by clinically significant bleeding. During this period of fluctuating platelet levels, the patient developed deep vein thrombosis of the right lower limb, leading to discontinuation of eltrombopag. In 2023, during intermittent use of a direct oral anticoagulant, the patient experienced a pulmonary hemorrhage, classified as major bleeding and requiring hospitalization.
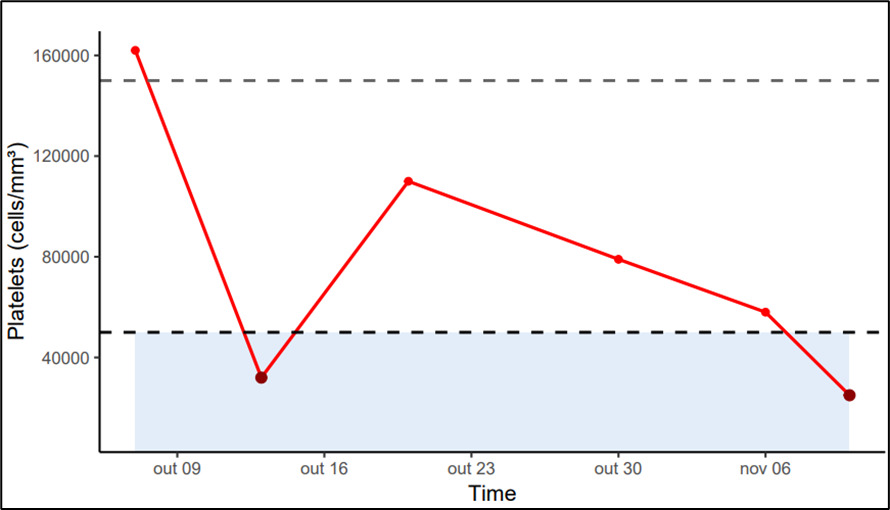
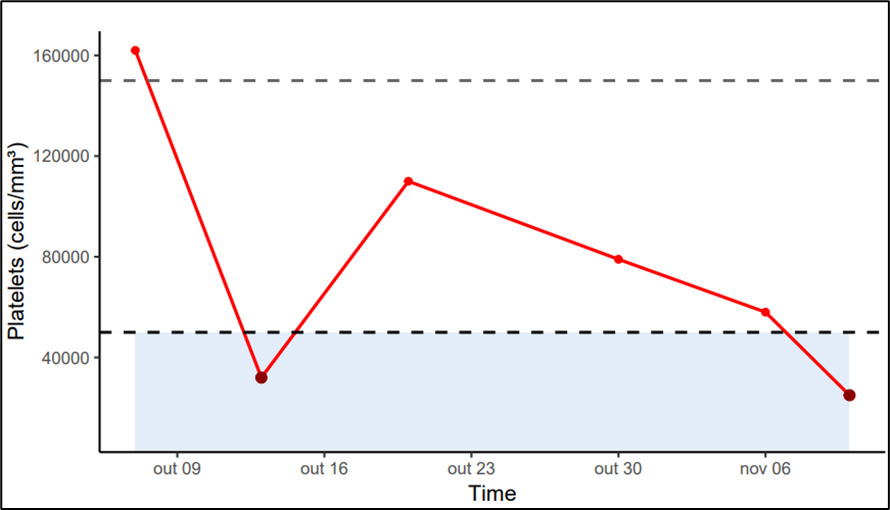
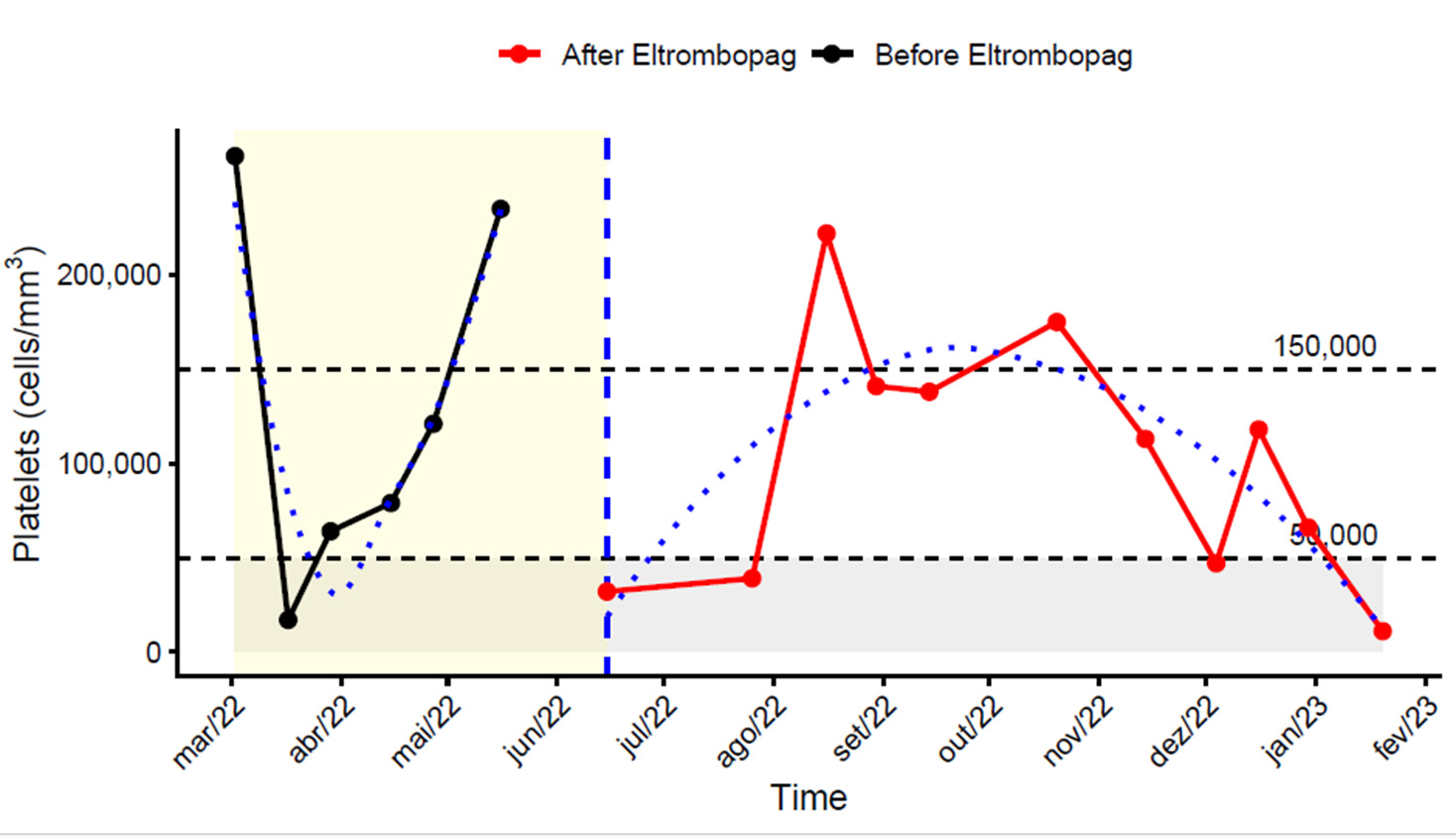
During evaluation at our service, marked platelet variability became evident, with counts fluctuating from less than 10,000/mm³ to over 100,000/mm³ within intervals of days to weeks. Notably, spontaneous cyclic recovery occurred approximately every 21 days, even in the absence of active treatment. A retrospective review of prior laboratory records revealed that this oscillatory pattern had been present since the early years following diagnosis but had not been previously recognized. No temporal association with the menstrual cycle was identified (Figure 1).
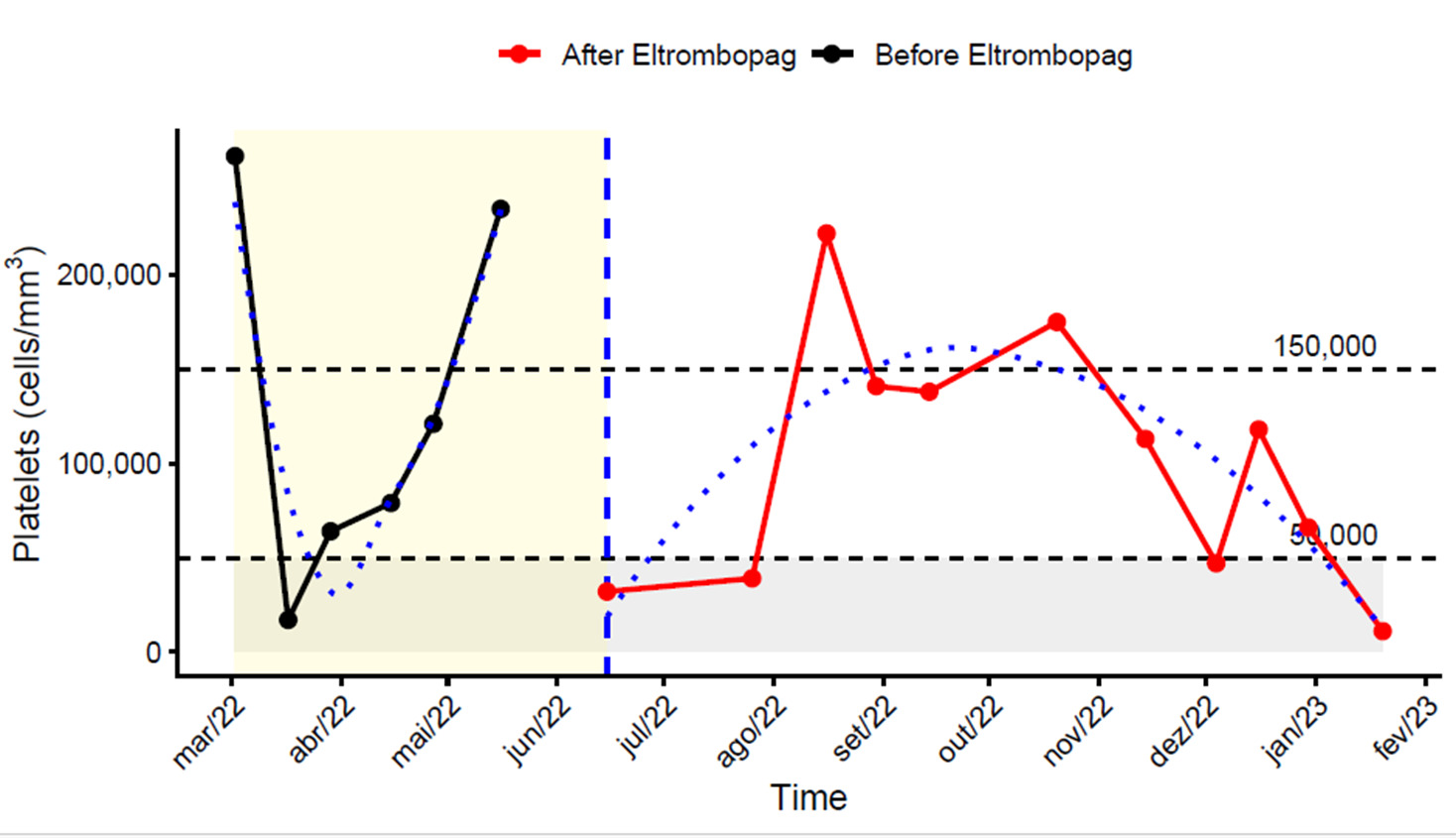
When platelet counts were evaluated immediately before and during eltrombopag therapy—the period in which the thrombotic event occurred—cyclic variability was still evident. However, the overall pattern appeared somewhat modified. Although fluctuations persisted, platelet counts remained above 100,000–150,000 cells/mm³ for longer intervals compared with the pre-treatment phase, as illustrated by the dotted trend line in Figure 2. Despite this apparent improvement, episodes of moderate-to-severe thrombocytopenia continued to occur, indicating that platelet stability was only partially achieved.
A comprehensive etiological investigation was performed, including viral serologies, autoimmunity tests, vitamin levels, and specialized hematological evaluations (PNH testing, myelogram, karyotype, and bone marrow immunophenotyping), all without evidence of a secondary cause or clonality. Given the characteristic laboratory pattern and the exclusion of alternative diagnoses, a diagnosis of cyclic thrombocytopenia was established. The consistent periodic oscillatory pattern, rather than persistent thrombocytopenia, supported the diagnosis of CTP over refractory ITP.
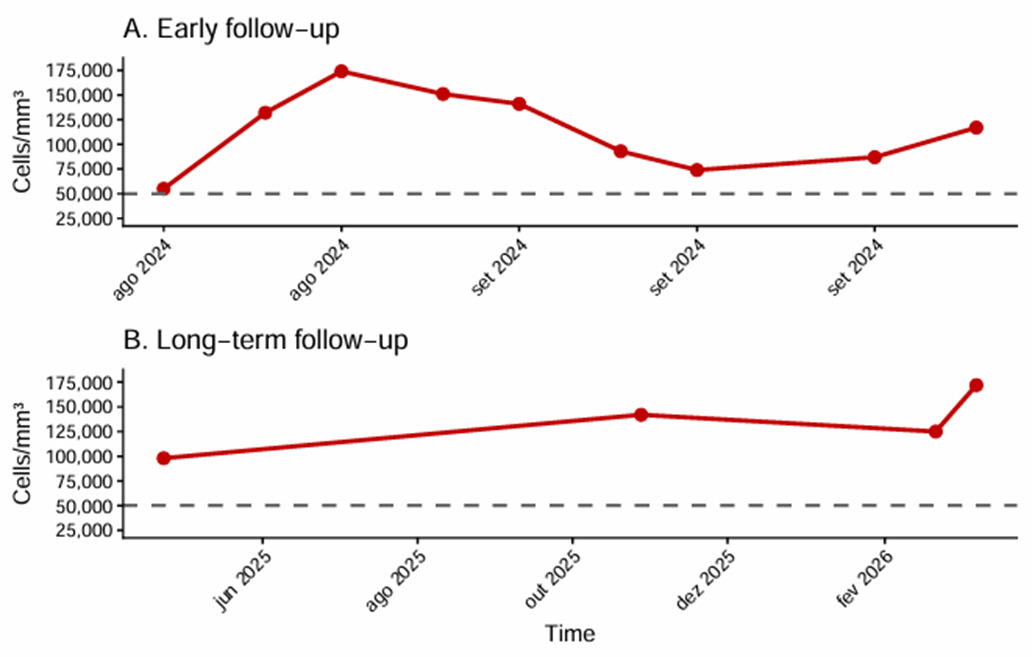
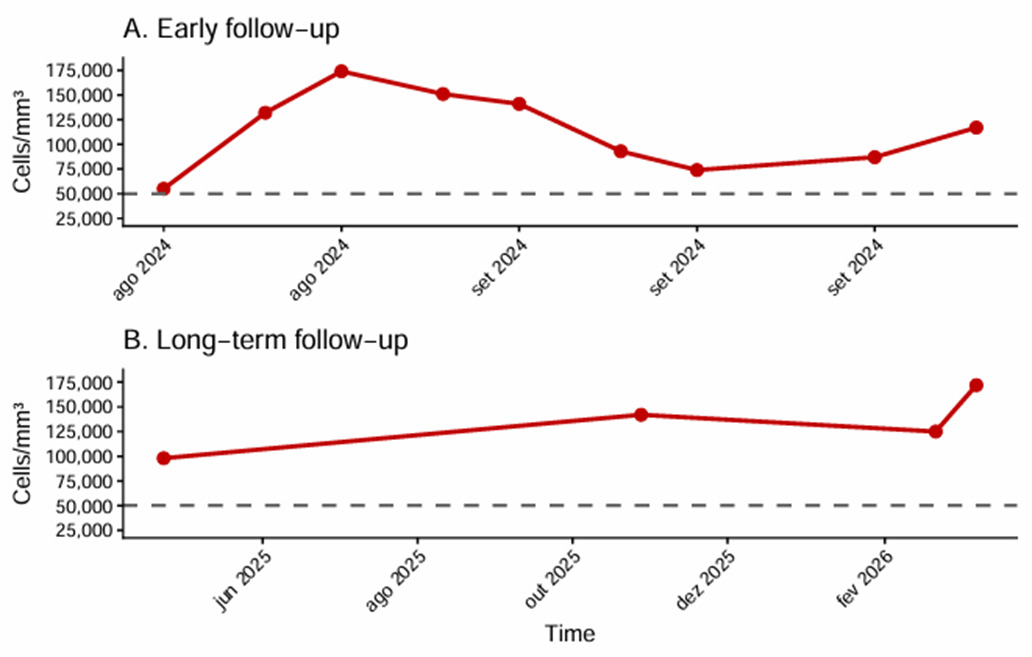
Given the refractory nature of the treatment, the history of thrombosis, and the high risk of bleeding, rituximab (375 mg/m² weekly for four weeks) was selected, concluding in June 2024. Following treatment, the patient showed a marked reduction in platelet oscillation amplitude, maintained platelet counts above 50,000 cells/mm³, and had no new clinical bleeding episodes. Clinical stability was sustained throughout short- and medium-term follow-up. As of the last evaluation in March 2026, the patient remained asymptomatic with platelet counts well above 50,000 (Figure 3).
Discussion
Cyclic thrombocytopenia is a rare and poorly understood disorder characterized by periodic oscillations in platelet counts, typically with cycles ranging from 3 to 5 weeks, followed by spontaneous recovery of platelet counts.4–6 This distinctive temporal pattern differentiates it from ITP, in which platelet decline is usually abrupt and follows a persistent or irregular course, with recovery occurring either spontaneously or in response to treatment, without a predictable cyclic pattern.7
The pathophysiology of cyclic thrombocytopenia remains incompletely understood, yet accumulating evidence suggests a predominantly immune-mediated mechanism, partially overlapping with pathways described in immune thrombocytopenia (ITP). Periodic peripheral platelet destruction appears to play a central role and may be accompanied by autoimmune targeting of megakaryocytes, leading to transient suppression of megakaryopoiesis. Autoantibodies directed against the thrombopoietin receptor have also been reported, supporting a dual pathogenic mechanism involving both impaired platelet production and enhanced peripheral destruction.3,4
In addition to humoral autoimmunity, cellular immune dysregulation has been proposed. Clonal T-cell receptor rearrangements have been described in selected cases, raising the possibility of an underlying immune clonal process and providing a rationale for observed responses to T-lymphocyte–modulating therapies such as cyclosporine.8 The marked predominance of cyclic thrombocytopenia among women of reproductive age further suggests a potential hormonal contribution to the cyclical modulation of platelet kinetics. Rare associations with infectious triggers have also been described, predominantly in experimental and animal models.3,4,9,10
In the acute setting, particularly during platelet nadirs associated with clinically significant bleeding, short-term immunomodulatory therapies such as corticosteroids and intravenous immunoglobulin (IVIG) may be considered. These interventions can transiently increase platelet counts and may provide temporary hemostatic control. However, unlike in immune thrombocytopenia (ITP), responses in cyclic thrombocytopenia are often inconsistent and short-lived, with no clear impact on the underlying cyclic pattern of platelet oscillation.4,5 In our case, prior exposure to corticosteroids did not result in sustained clinical benefit, reinforcing the limited role of these therapies as long-term management strategies in CTP.
In this case, persistent bleeding prompted the initiation of eltrombopag. However, the patient subsequently developed deep vein thrombosis despite the absence of thrombocytosis, with a maximum platelet count of 258,000 cells/mm³. This observation aligns with previous reports suggesting that the thrombotic risk associated with TPO receptor agonists is not solely dependent on elevated platelet counts.1 In addition to quantitative increases, these agents may contribute to qualitative platelet activation and enhanced endothelial interactions, potentially promoting thrombosis even when platelet levels remain within the normal range.1,11 This clinical course underscores the paradoxical nature of cyclic thrombocytopenia, in which hemorrhagic and thrombotic risks may coexist at different phases of platelet oscillation.
Therapeutic management of CTP remains challenging due to the rarity of the condition and the absence of randomized clinical trials. Available evidence from observational studies and case series suggests that CTP is frequently refractory to conventional therapies used in immune thrombocytopenia or achieves only transient responses. Given its predominantly immune-mediated pathophysiology, immunomodulatory therapies such as rituximab represent a plausible therapeutic approach, although reported responses are often partial.2,6 In this context, the novelty of our case lies in the unique clinical scenario and observed outcomes, including sustained response through the last evaluation in March 2026, rather than in the use of rituximab itself.
The partial stabilization observed after rituximab may support an immune-mediated mechanism underlying the cyclic pattern in this patient. In this report, the patient showed a satisfactory clinical response to rituximab, maintaining the oscillatory pattern of platelet count, but with a consistent increase in the platelet nadir to values above 50,000 cells/mm³. This finding led to a significant reduction in bleeding episodes, greater clinical safety, and substantial improvement in quality of life, reinforcing the role of rituximab as a relevant therapeutic alternative in selected cases of symptomatic and refractory thrombocytopenia.
This case highlights a prolonged diagnostic delay, retrospective identification of a consistent cyclic platelet pattern, the coexistence of thrombotic and hemorrhagic complications associated with thrombopoietin receptor agonist therapy, and a clinically meaningful response to rituximab characterized by reduced oscillation amplitude and stabilization of platelet nadirs above clinically significant thresholds. These findings may contribute to a better understanding of treatment selection and risk stratification in complex cases of CTP.
Other alternative treatments such as danazol and cyclosporine have been reported for CTP, primarily in isolated case reports and small series. Danazol, especially in female patients, has been associated with platelet stabilization, possibly through hormonal and immunomodulatory mechanisms, while cyclosporine targets T-cell–mediated immune pathways. However, both options have significant limitations due to adverse effects and long-term toxicity. In this case, these therapies were not chosen as initial options because of the patient’s history of thrombotic events and the known prothrombotic and metabolic risks of danazol, as well as the nephrotoxic and infectious risks of cyclosporine.12
Conclusion
Cyclic thrombocytopenia is a rare but clinically significant disorder whose clinical features frequently overlap with those of immune thrombocytopenia, leading to diagnostic delays and increased morbidity.13 Therapeutic management remains challenging due to the limited quality of available evidence. In this context, our findings suggest that rituximab may represent a therapeutic option in carefully selected, refractory cases, although further studies with more robust methodological designs are required to better define its efficacy and safety in cyclic thrombocytopenia.
Disclosures/Conflicts of Interest
The authors declare that they have no conflicts of interest.
Corresponding Author
Jandir Mendonça Nicacio MD, MSc, PhD
Professor, School of Medicine,
Universidade Federal do Vale do São Francisco -UNIVASF, Petrolina (PE), Brazil
Email: jandir.nicacio@univasf.edu.br