Background
Powassan virus (POWV), an emerging flavivirus transmitted by the Ixodes tick, has become increasingly concerning due to its potential to cause severe neurological conditions, including encephalitis and meningitis, in humans. Initially discovered in the 1950s, the number of reported cases of POWV has been rising, especially in the northeastern regions of the United States. Between 2004 and 2024, roughly 400 confirmed cases were reported to the Centers for Disease Control and Prevention (CDC).1 Of these, 377 were classified as neuroinvasive, 371 necessitated hospitalizations, and 53 ended in death.1 Despite increasing recognition, POWV virus infection remains underdiagnosed due to its nonspecific prodromal symptoms and limited availability of rapid diagnostic testing, often requiring confirmation through state health departments or the CDC. The mechanism by which POWV crosses the blood-brain barrier remains unclear but has been hypothesized to occur via infected immune cells, passively via infection of the blood-brain barrier, or actively by disrupting blood-brain barrier endothelial cell tight junctions.2
Infected individuals are typically asymptomatic during an incubation period from 1 to 5 weeks.3 A brief prodromal phase may follow, characterized by fever, myalgias, weakness, headache, and sore throat. Neurological manifestations can develop weeks to months later and commonly include fever, altered mental status, decreased consciousness, and seizures.3 Diagnosis is primarily based on serological testing for immunoglobulin M (IgM) antibodies, typically performed by state health departments or the CDC. Radiographic and clinical features of POWV encephalitis frequently overlap with other viral encephalitides, including West Nile virus and herpes simplex virus, further complicating early diagnostic differentiation. With no specific antiviral treatment or vaccine available, management relies heavily on supportive care. This report addresses a particularly severe case of POWV encephalitis in an elderly patient, underscoring the public health concerns and importance of suspecting POWV in cases with a history of tick-borne neuroinvasive disease.
Case Presentation
A 77-year-old white female with a medical history of hypertension, hyperlipidemia, chronic obstructive pulmonary disease, gastroesophageal reflux disease, and depression. She was an active individual living in a rural area in Connecticut, known for outdoor activities such as gardening. Approximately three weeks before her presentation, the patient removed several ticks embedded in her skin and subsequently completed a three-day course of cephalexin. She presented with fever, mild weakness, and dragging of her left leg upon waking. She denies any recent travel history. On examination, the patient was lethargic with absent movement in her left upper and lower extremities. She also displayed a right facial droop with an asymmetric smile, although she could close her eyes and furrow her brow symmetrically. There were no other cranial nerve deficits. Her cardiovascular examination was notable for tachycardia with a regular rhythm. The patient also showed nuchal rigidity, indicative of potential meningeal irritation, and has a right gaze preference with the ability to visualize the left field of vision. Vital signs indicated a pulse of 102/min, respiration rate of 24/min, blood pressure of 170/74 mm of Hg, and oxygen saturation of 90% on room air. The patient’s temperature ranged between 100.3°F and 105°F. Subsequently, the patient’s weakness rapidly progressed from hemiparesis to quadriparesis over three days. The patient also developed worsening lethargy requiring mechanical ventilation for airway protection.
Laboratory tests showed elevated liver function tests (AST/ALT 100/96 IU/L), leukocytosis (16.1 x 10^3/μL), normal platelet count (220,000/μL), and mildly elevated procalcitonin. Comprehensive tick and viral panels were performed. Serological studies were negative for Lyme IgG/IgM antibody, Rocky Mountain Spotted Fever (RMSF) IgG/IgM, Babesia microti NAA (Nucleic Acid Amplification), Anaplasma phagocytophilium NAA, Ehrlichia chaffeensis NAA, and Human Immunodeficiency Virus (HIV). Cerebrospinal fluid (CSF) evaluation from lumbar puncture revealed pleocytosis (leukocytes 76/μL with 87% lymphocytes, 1% neutrophils, and 12% monocytes) and elevated protein levels (130 mg/dL). CSF polymerase chain reaction (PCR) was negative for common bacterial [Escherichia coli K1, Haemophilus influenzae, Listeria monocytogenes, Neisseria Meningitidis, Streptococcus agalactiae, Streptococcus pneumoniae], viral [Cytomegalovirus (CMV), Enterovirus, Herpes Simplex Virus (HSV) 1 and 2, Human Herpesvirus 6 (HHV-6), Human Parechovirus, Varicella Zoster Virus (VZV)], and Cryptococcus neoformanns/gatti. CSF was negative for autoimmune and paraneoplastic antibody panel. Further tests were requested to check for Eastern equine encephalitis (EEE) virus and Powassan virus at the state department of health. The CSF Powassan virus IgM antibody was positive, confirming the diagnosis. Further confirmatory testing was done by forwarding the sample to the CDC.
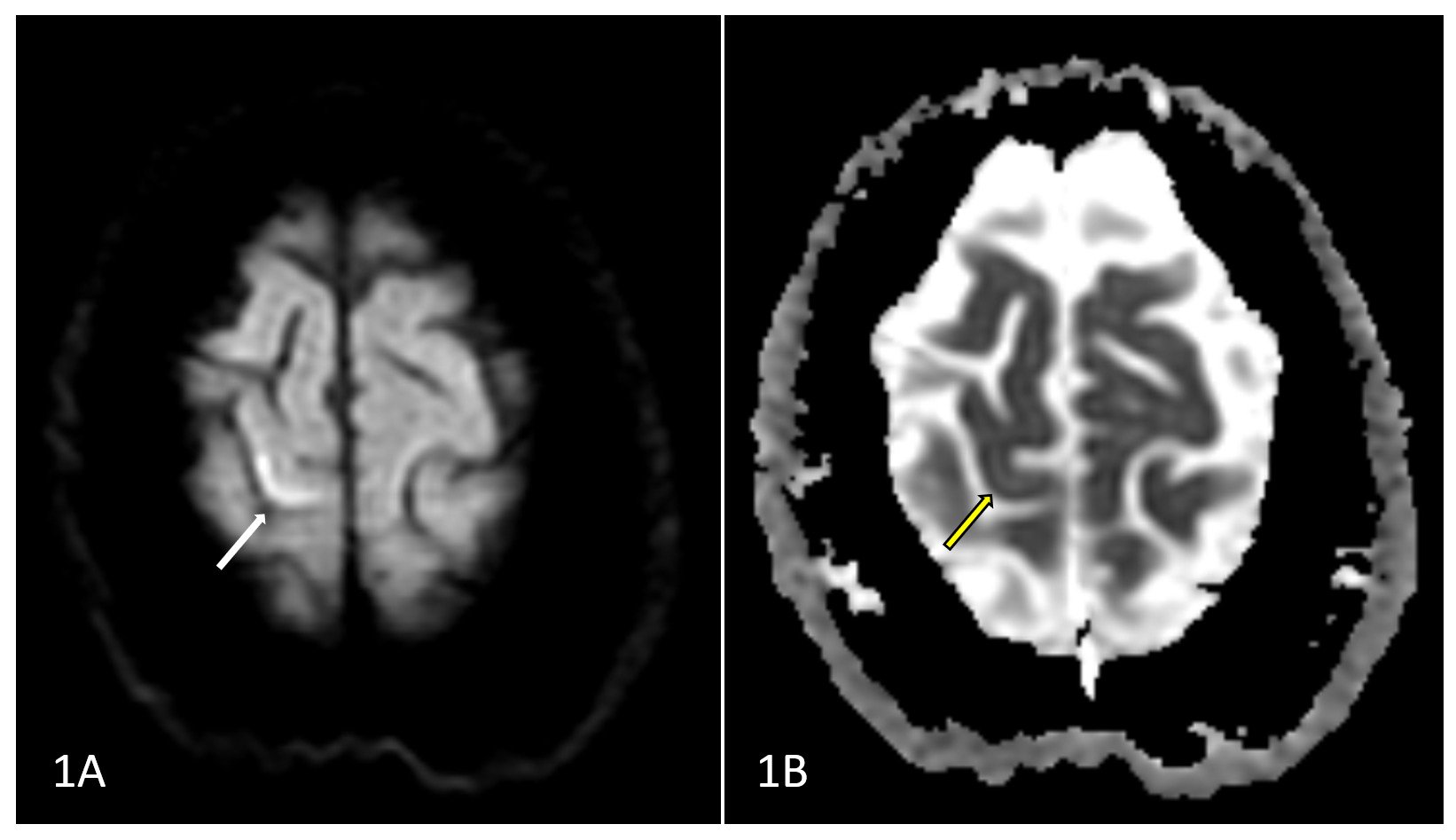
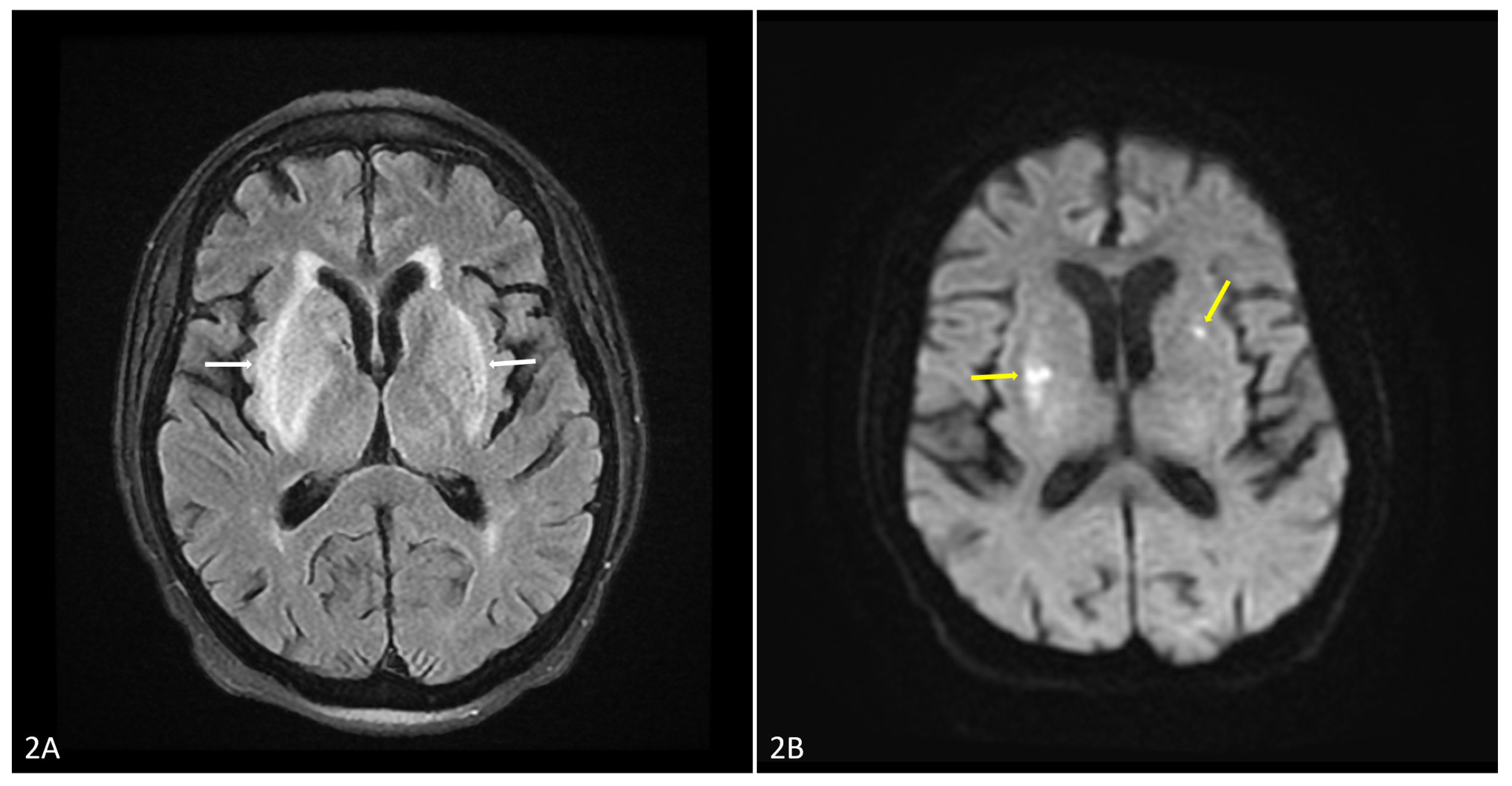
Magnetic resonance imaging (MRI) at presentation demonstrated focal diffusion restriction in the medial right precentral gyrus, corresponding to the primary motor cortex, raising concern for acute ischemic infarction (Figure 1). The same study also demonstrated T2/FLAIR hyperintensities in the basal ganglia, more pronounced on the right, which were atypical for a single vascular territory infarction. Repeat MRI performed three days later demonstrated progression with worsening bilateral basal ganglia abnormalities and additional multifocal cortical, cerebellar, and brainstem involvement (Figure 2). Diffusion restriction persisted within the right precentral gyrus and developed within portions of the basal ganglia and cerebellum. The evolving pattern of multifocal bilateral deep gray matter and infratentorial involvement favored an infectious or inflammatory encephalitic process rather than isolated vascular pathology. Initial differentials included acute ischemic stroke, bacterial meningitis, viral encephalitis, and autoimmune encephalitis. The factors supporting and refuting each diagnosis, along with the diagnostic tests performed, are summarized in Table 1. Given the patient’s clinical picture and exposure history, POWV encephalitis was suspected and confirmed with specific serologic testing.
_demonstrating_focal_cortical_diffusion_restri.png)
_demonstrating_progression_to_bilateral_deep.png)
The patient was initially managed with dual antiplatelet therapy and statins due to the concern of a stroke. As her condition progressed, broad-spectrum intravenous (IV) antibiotics such as ceftriaxone and vancomycin, and IV antivirals such as acyclovir, were administered until the POWV was confirmed. After confirmation, treatment focused on supportive care, including mechanical ventilation, seizure prophylaxis with Levetiracetam, and hemodynamic support with intravenous fluids and vasopressors as needed. Sedation with propofol and aspiration precautions were also employed while on mechanical ventilation. Despite aggressive supportive care, the patient’s condition continued to decline. She developed aspiration pneumonia and remained ventilator dependent. Given the severity of her encephalitis and poor prognosis, her family decided to transition her to comfort measures only. She was subsequently admitted to inpatient hospice care, where she expired.
Discussion
This case of POWV encephalitis in an elderly female who presented with relatively mild neurological symptoms, which swiftly escalated into severe encephalopathy and quadriparesis. The rapid progression to severe encephalitis highlights the challenges in managing POWV infections, which often present with non-specific symptoms that mimic other more common conditions like ischemic stroke or viral encephalitis due to HSV or WNV. This case reinforces that early diffusion-weighted MRI abnormalities do not exclude infectious or inflammatory etiologies and that clinicians should consider POWV encephalitis among stroke mimics in endemic regions.
In a systematic review of 84 POWV cases in North America and Canada, complications such as paralysis (most commonly hemiplegia) were observed in 44.1% of patients and cognitive deficits in 33.3% of patients.4 The study identified significant positive correlations between mortality and factors such as old age, development of paralysis, and respiratory distress or failure: all of which were present in this case. Comparative case reports and case series, such as those by Solomon et al,5 Mendoza et al,6 Cavanaugh et al,7 and Johnson et al,8 illustrate similar clinical trajectories, with many patients requiring intensive care and mechanical ventilation, and emphasize the microbial virulence, leading to high mortality rates and significant neurological sequelae in survivors.
T2/FLAIR hyperintensities are a common MRI finding associated with POWV encephalitis and were found in the basal ganglia, gray matter, and cerebellum of this patient. Cerebellar involvement has been associated with more severe disease and poorer clinical outcomes. Although these findings are not specific to POWV and found in other arboviral encephalitides, prior case reports and series have documented T2/FLAIR hyperintensities in almost all reported cases of POWV.4,9,10 Unlike HSV encephalitis, which classically involves the temporal lobes, POWV more commonly affects deep gray matter structures, including the basal ganglia and thalami. These findings have been described throughout the brain, with a predilection for deep gray matter structures such as the basal ganglia.4,9,10 In this patient, acute ischemic infarction was initially suspected due to focal cortical diffusion restriction and lateralized neurological deficits; however, the presence of concurrent and progressive bilateral basal ganglia abnormalities was atypical for infarction confined to a single vascular territory. Together with our findings, these studies emphasize the importance of considering arboviral encephalitides, including POWV encephalitis, in patients with T2/FLAIR hyperintensities on MRI and a relevant history of tick exposure in endemic areas. Herpes simplex virus encephalitis was considered less likely given the absence of predominant temporal or limbic involvement.11
From an imaging perspective, Creutzfeldt-Jakob disease (CJD), autoimmune encephalitis, and metabolic or toxic etiologies, including hypoglycemia, mitochondrial disorders, and carbon monoxide poisoning, were also considered.12 However, the rapid progression and multifocal cortical and infratentorial involvement were less characteristic of these entities. Overall, the distribution and evolution of imaging abnormalities, together with clinical and laboratory findings, supported a diagnosis of infectious encephalitis. This case underscores the importance of early recognition and diagnosis of POWV, especially in endemic areas with high tick exposure.
Public health measures to prevent tick bites, particularly in endemic areas, are crucial in mitigating the risk of this emerging infectious disease. Clinicians should maintain a high index of suspicion for POWV in patients presenting with encephalitis symptoms and a history of tick exposure, even considering the inclusion of POWV in tick-borne disease panels. While the initial treatment strategy was appropriate, the absence of specific antiviral therapies highlights a significant gap in the management of POWV encephalitis, reinforcing the need for further research and development in this area. Notably, POWV transmission may occur within minutes of tick attachment, emphasizing that prompt tick removal alone may not prevent infection and reinforcing the importance of preventive public health measures.
Disclosure/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding author
Sushrut Ingawale MD, DNB, MBBS
Department of Internal Medicine,
Quinnipiac University - Frank H Netter, MD School of Medicine/St. Vincent’s Medical Center
Email: drsushrutingawale@gmail.com