Background
The Accreditation Council of Graduate Medical Education (ACGME) requires that all residents demonstrate the ability to perform “all medical, diagnostic, and surgical procedures considered essential for the area of practice.”1 The American Board of Internal Medicine (ABIM), further clarifies that the specific procedures that residents should gain competency in are flexible, guided by the specific residency program and the resident’s anticipated career path, rather than a predetermined list of procedures.2 In a survey of fellowship program directors, many directors reported preferring that graduating residents enter fellowship already competent in multiple procedures.3
Residents commonly learn bedside procedures from peers, faculty members, or ancillary staff, either during clinical rotations or in an elective/procedure team setting. Reliance on faculty members as instructors and supervisors can be challenging due to the limited availability of faculty champions.4–6 There is no standardized method or guidelines for teaching bedside procedures. Meta-analyses evaluating bedside procedure curricula found that simulation is the most frequently used modality, though session duration, frequency, and structure can vary greatly.7,8 Most studies assess the positive impact on resident confidence.7,9–16 Few studies, primarily interventions centered around procedure rotations, evaluate clinical outcomes such as procedure volume9,17–20 or the number of needle passes required.9,10 Even fewer are noted to report complication rates.6,7,20 Beyond meeting resident milestones and educational goals, proficiency in bedside procedures has been shown to reduce healthcare costs21–23 and shorten the length of time to procedure22 compared with consulting services such as interventional radiology.
The procedural training workshop (PTW) was designed and implemented to provide standardized procedural education for internal medicine residents through simulation. We hypothesized that participation in the PTW would increase resident confidence and independence in performing bedside procedures and translate to increased bedside procedures volume with maintenance of high success rates and low complication rates.
Methods
Setting and Participants
All first-year and second-year residents in the internal medicine residency at Brown University in Providence, Rhode Island were assigned to complete a half-day PTW held at a simulation center affiliated with the medical school. Instructors were comprised of faculty, pulmonary-critical care fellows, chief residents, and senior residents who were “signed-off” to perform the procedure, defined as having successfully completed at least 5 procedures under direct supervision and demonstrating comfort performing the procedure independently.
Pre-Workshop
A flipped classroom model was used, with residents receiving instructional slides and New England Journal of Medicine procedural videos prior to the PTW.24–26 These resources outlined procedural steps, risks and benefits, contraindications, troubleshooting tips, and hospital-specific workflow pearls. Materials were also reviewed with station instructors before the workshop to ensure standardized teaching across stations. Residents were assigned to one of sixteen half-day PTW sessions during elective or primarily ambulatory rotations to ensure adequate time to review the materials. Two half-day PTW sessions, run consecutively within a single day, were held each month from September through April. Priority was given to schedule residents prior to critical care rotations to allow for exposure of central line placement prior to clinical use.
Workshop Timeline
On the day of the workshop, residents rotated through three stations with ultrasound-compatible task trainers for lumbar puncture (LP), paracentesis, and central venous catheter (CVC) placement. Each station had a maximum of a 2:1 resident-to-instructor ratio. At each station, residents performed each procedure at least once and had the opportunity to ask instructors about troubleshooting techniques. Static ultrasound guidance was taught for paracentesis and lumbar puncture, while dynamic guidance was taught for central venous catheter placement. Each station was allotted 45 minutes.
Evaluation
Upon arrival at the simulation center on the day of the PTW, residents completed a pre-session 14-question multiple-choice knowledge test on basic procedural troubleshooting and time-out techniques, along with a pre-session survey on self-rated preparedness and independence. Questions were aligned with the session’s learning objectives and tested concepts such as components of a time-out, identification of a safe ascitic fluid pocket for paracentesis, patient positioning for measurement of CSF opening pressure, and appropriate management when a post-CVC placement x-ray reveals an improper catheter tip location. Immediately after the stations, residents completed a similar post-session knowledge test and attitudes survey. To quantify number of procedures performed by internal medicine residents, standardized procedure notes authored by internal medicine residents, which document success, attempts, and complications, were collected via Epic’s Reporting Workbench function and were analyzed from the year prior to implementation (2020-2021), the first year of implementation (2021-2022), and the fourth year of implementation (2024-2025) from the two main teaching hospitals.
Statistical Analysis
Chi-square was used to analyze all categorical variables. Student’s T-test was used to compare average test scores. A p-value of <0.05 was considered statistically significant. All statistics were run using Statistical Package for Social Sciences (SPSS) Version 27, (IBM Corporation, Armonk, New York) and StatPlus version 7 (AnalystSoft, Alexandria, VA, US). This study was deemed as exempt by the Brown University Health IRB.
Results
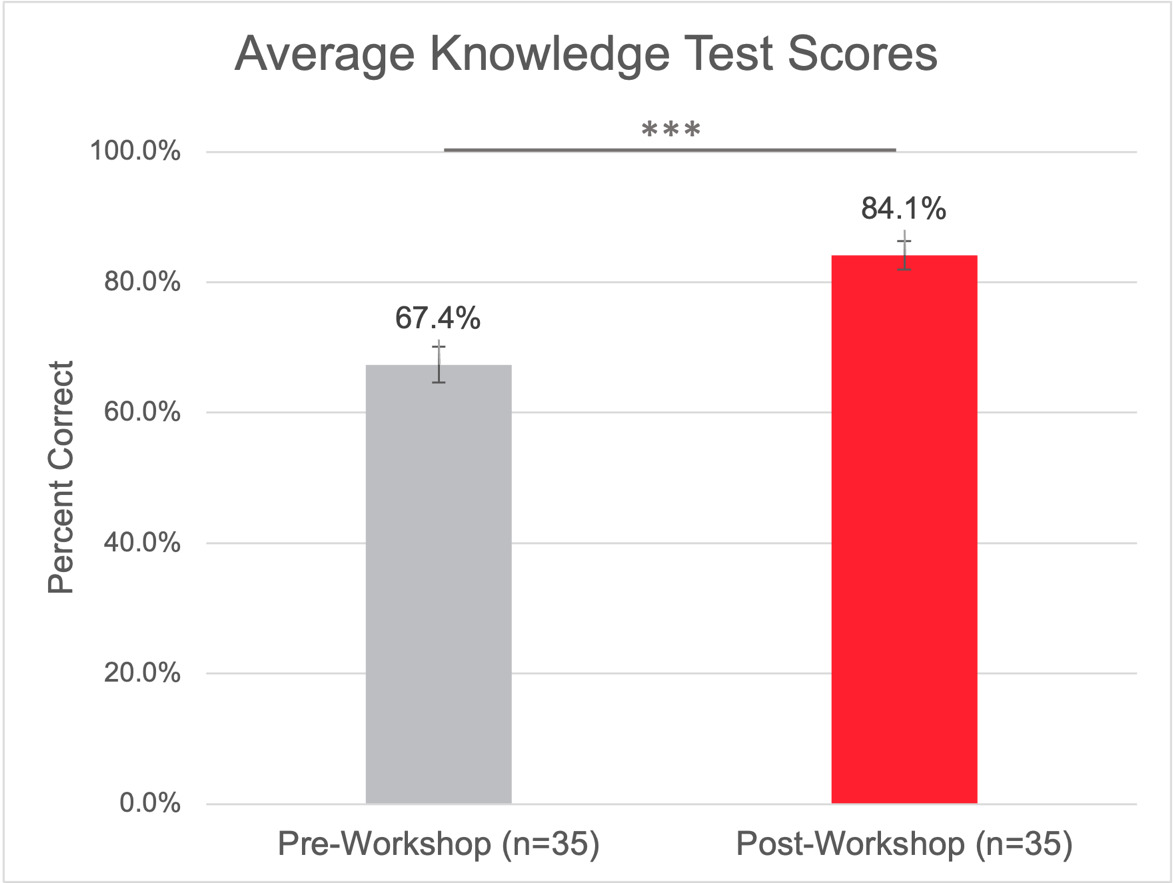
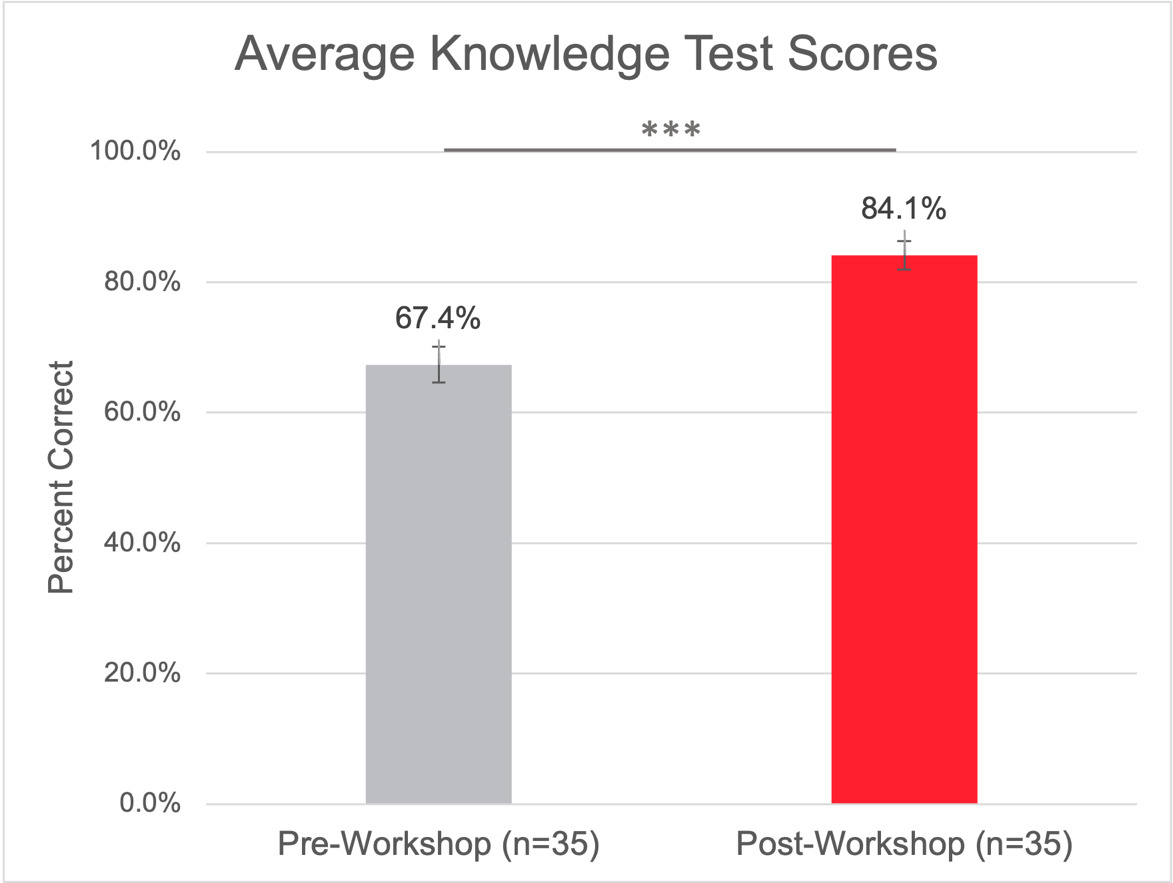
In 2021, the first year of implementation, there were 35 participants in the PTW with 46% first-year residents and 54% second-year residents. When comparing pre-PTW and post-PTW knowledge test scores, there was an increase from 67.4% ± 16.4% to 84.1% ± 13.1% (p <0.001, Figure 1).
Regarding attitudes and beliefs, residents reported increased preparedness (Table 1) and independence (Table 2) when performing the procedures. The proportion of residents feeling “well-prepared” to perform or “teach others” rose for paracentesis (from 28% to 80%, p < 0.05), LPs (from 8% to 71%, p <0.05) and CVC placement (from 31% to 69%, p < 0.01). Similarly, those reporting they could perform all steps without assistance or model for others increased for paracentesis (from 25% to 66%, p < 0.01), LP (from 17% to 49%, p < 0.01), and CVC placement (from 28% to 54%, not statistically significant).
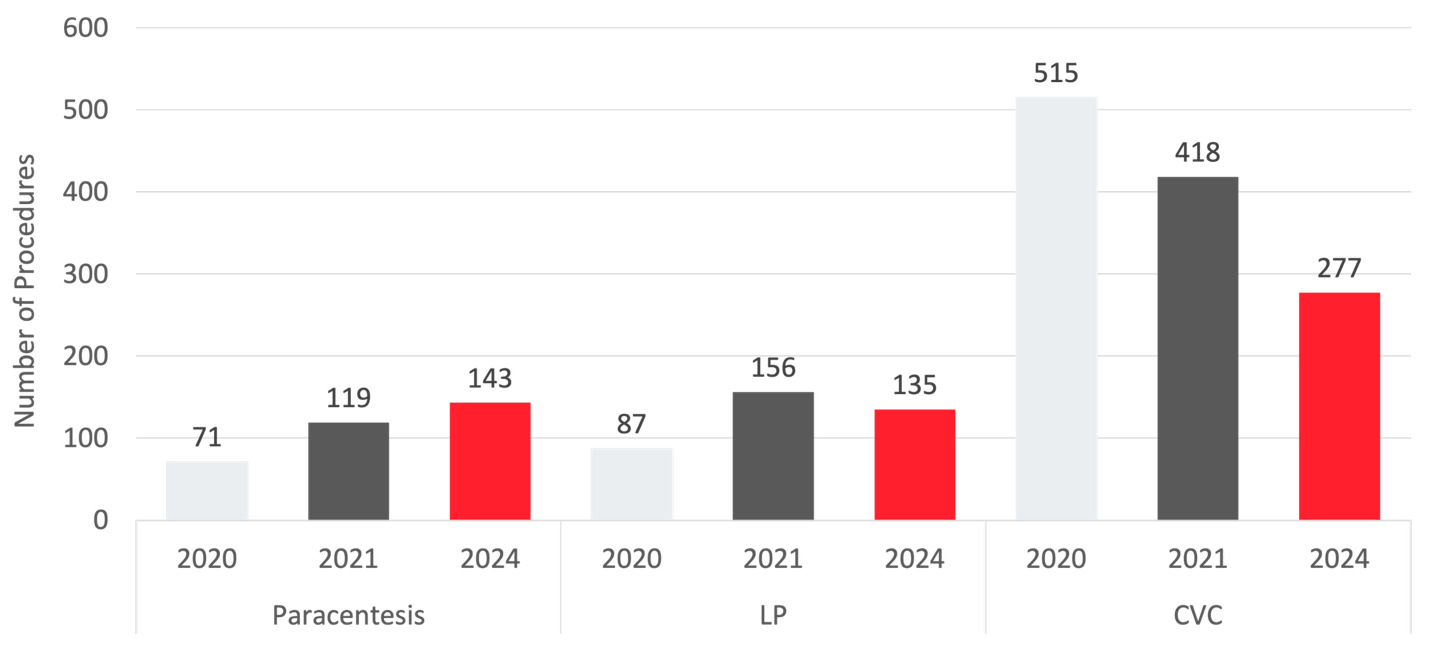
When comparing the number of procedures from 2020 to 2021 to 2024, there were increases in paracenteses from 71 to 119 to 143 and LPs from 87 to 156 to 135 (Figure 2).
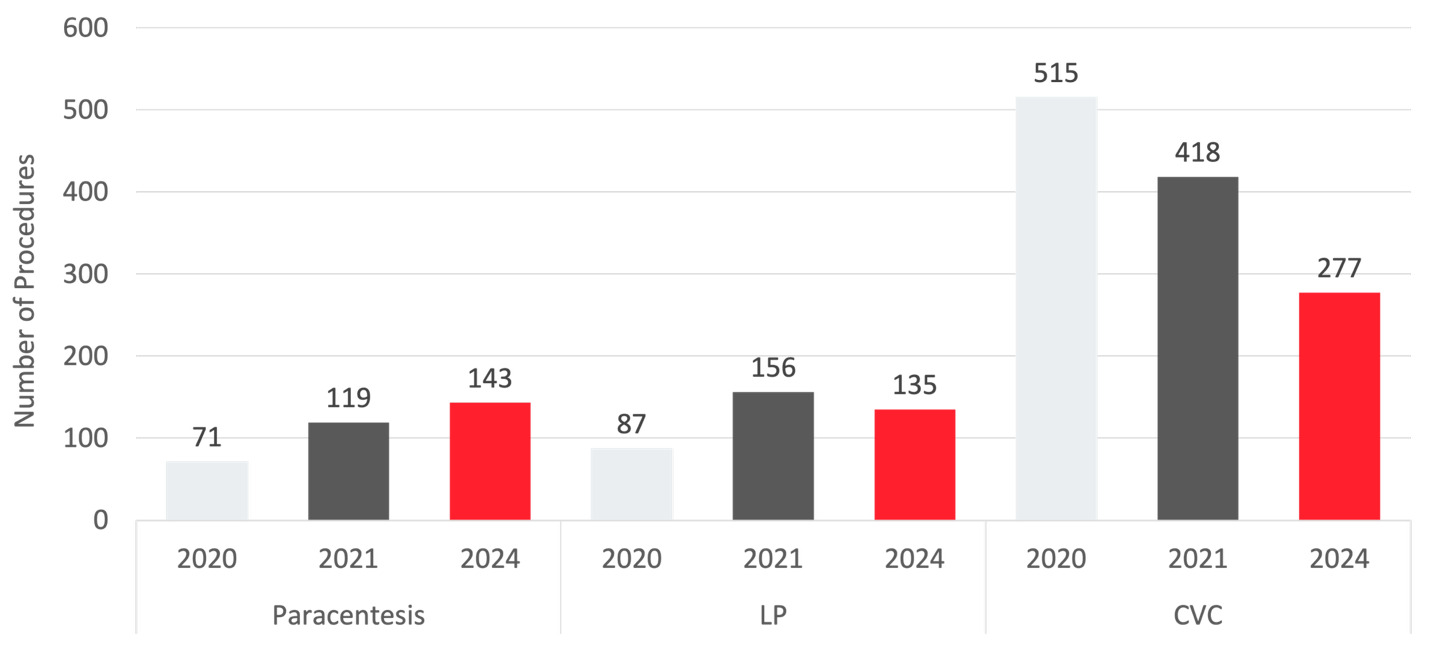
Notably, the number of CVCs decreased since 2020 from 515 to 418 to 277. There were similar success rates across all three years (Table 3): 91.5% to 94.1% to 93.7% for paracentesis with X2 (2, N = 333) = 0.056, p = 0.45, 58.6% to 55.8% to 52.6% for LPs with X2 (2, N = 378) = 0.65, p = 0.42, and 95.5% to 97.6% to 94.9% for CVC with X2 (2, N = 1210) = 3.97, p = 0.046. There were also similar rates of immediate post-procedural complications that were not statistically different (Table 3), 0.0% to 0.8% to 2.8% for paracentesis with X2 (2, N = 333) = 3.06, p = 0.080, 2.3% to 1.9% to 0.0% for LP with X2 (2, N = 378) = 2.88, p = 0.090, 2.7% to 1.2% to 2.2% for CVC placement with X2 (2, N = 1210) = 2.66, p = 0.26. Documented complications were minor with minimal medical intervention required and included localized hematoma for CVC placement and ascitic fluid leakage and intra-procedural hypotension for paracentesis.
Discussion
After participation in the PTW, residents demonstrated immediate increases in knowledge and self-reported confidence, comparable to results reported in the literature for other procedural training programs.9,11,12 Knowledge gains were greatest for paracentesis and LPs, while scores for CVC placement and time-outs questions remained high both pre- and post-PTW. This likely reflects the relative unfamiliarity residents have with paracentesis and LPs early in training.27 Increases in self-reported preparedness and independence mirrored effects seen in other procedural interventions.9–15
Clinical data revealed sustained increases in volume of paracentesis and LPs from 2021 (the year of implementation) to 2024. This is a similar trend to what has been reported with procedure rotations, specifically that procedural volume increased with continued implementation of the programs and is likely due to the increased pool of residents who felt comfortable independently performing the procedures.9,17–19 At our institution, a common barrier to bedside procedures prior to PTW implementation was residents’ difficulty identifying a qualified supervisor. Faculty comfort with bedside procedures was variable, and residents often relied on senior residents for direct supervision; without a supervisor, they frequently had to consult interventional radiology to perform the procedure. Senior residents, after completing at least five procedures under direct supervision and demonstrating proficiency, became eligible to perform procedures with indirect faculty supervision and to supervise junior residents. Expanding the pool of senior residents with procedural independence increased junior residents’ exposure to and comfort with bedside procedures, supporting their progression toward independent practice. In contrast, CVC insertion numbers decreased from 2020 through 2024, likely reflecting increased CVC utilization for critically ill patients during the COVID-19 pandemic, consistent with larger epidemiologic studies.28
Despite higher volumes of paracentesis and LPs, success and complications rates remained stable. Complications rates of all three procedures (0-2.8%) were comparable to published data (paracentesis 0.5-10.8%,29–32 LPs 0.0-3.4%,31–33 CVC placement 0.3-11.6%31–35). Notably, there was a nonsignificant increase in immediate post-procedural complications after paracentesis. Documented complications in 2024 were persistent post-procedural ascitic fluid leakage (3 out of 143), which resolved with either placement of an ostomy bag or use of sutures to close the entry point and intra-procedural hypotension (1 out of 143). Studies have noted variable risk of paracentesis leak from 0-23%.29 The procedure form template has an optional free-text area for noting post-procedural complications. As procedure training has become embedded within the residency curriculum, documentation has likely improved, which can lead to better identification and reporting of even minor complications. Other documented complications for CVC placement included localized hematoma and incorrect location of line. Success rates for paracentesis and CVC align with prior reports—paracentesis (91.5-94.1% vs. 95%36) and CVCs (94.9-97.6% vs. 96%35). Lower LP success rates (52.6-58.6% vs. 73.0-90.0%6,31,37,38) may be explained by inherent procedural challenges or patient factors including body habitus38–40 or prior spine surgery38 that impact the likelihood of success and need for current simulation training to more fully replicate clinical conditions. Additionally, due to interventional radiology scheduling constraints, bedside attempts were often undertaken to advance the care plan, even when the aforementioned patient factors heightened the likelihood of failure.41 Another factor likely contributing to the lower success rates is the relatively low use of ultrasound-assisted LPs, whereby the optimal needle insertion site is identified by precisely locating the midline of the spine and the largest interspinous space. Although ultrasound-assisted LPs are taught during the PTW, most LPs performed by residents are still performed by palpation of surface landmarks due to limited availability of ultrasound machines on the general medical floors. Gottlieb, et al found that ultrasound-assisted LPs increased success rates, decreased rates of traumatic LPs, decreased time-to-complete procedure, and decreased mean needle passes.37 Improving resident access to ultrasound machines and emphasizing routine use of ultrasound-assisted LPs may improve success rates and procedural efficiency.
Strengths of this intervention include the use of senior residents and pulmonary critical care fellows as instructors, which reduced the reliance on attendings physicians and enabled maintenance of low learner-to-instructor ratios. This structure allowed residents increased hands-on-practice time42 and provided greater flexibility in scheduling. Teaching was standardized across stations through pre-session instructor preparation, improving consistency in content and expectations. Additionally, the longitudinal nature of this intervention, requiring both first-year and second-year residents to participate, supported long-term retention of skills and progression towards procedural independence.
This study had several limitations. The study used a historical control, data from 2020, as the point of comparison, which limits the ability to control for bias such as selection bias. While there were increases in immediate recall as noted by the knowledge assessment, there was no assessment of long-term recall. Additionally, while residents self-reported they felt prepared to teach the procedure, there was no formalized assessment of this. The PTW was conducted at a single internal medicine training program with access to a simulation center with ultrasound-compatible task centers, which may limit generalizability to programs without such resources. For example, the reliance on senior residents and fellows as instructors may be a limiting factor for programs with fewer trainees. Post-procedure documentation variability is another limitation; while certain fields are required in procedure notes, the level of detail remains at the residents’ discretion, leading to possible underreporting of outcomes, including complications. This study design also does not account for long-term complications, such as catheter line-associated bloodstream infections.
Conclusions
The procedure training workshop is an effective half-day longitudinal intervention for teaching residents’ bedside paracentesis, LPs, and CVC insertion. By recruiting senior residents and fellows, in addition to faculty, the PTW can be run multiple times a year to reach all first- and second-year residents while maintaining a low learner-to-instructor ratio. The PTW not only increased residents’ knowledge, independence, and confidence but also increased the number of bedside procedures performed with high success and low complication rates, making it an overall effective modality for teaching and reinforcing bedside procedures.
Acknowledgments
The authors would like to acknowledge the help and support of the Brown Internal Medicine residents, attendings, and pulmonology fellows for volunteering as instructors. The authors would also like to thank the department’s administrative staff for their continued help with scheduling and logistics of the workshop. The authors would also like to thank Khalil Ahmad, M.Sc., MPhil, for his help with statistics.
Disclosures/Conflicts of Interest
The authors have no disclosures.
Corresponding author
Cynthia Zheng, MD
Chief Resident, Department of Internal Medicine
593 Eddy St, Room 0100, Providence, Rhode Island 02903
Email: czheng@brownhealth.org