Background
Electroconvulsive therapy remains one of the most effective treatments for severe, refractory mood disorders. It is generally regarded as safe, with a low incidence of adverse cardiovascular events. However, ECT can induce acute hemodynamic changes, including transient bradycardia followed by marked sympathetic activation with tachycardia, hypertension, and elevated circulating catecholamines.1 Given this, in some patients, serious cardiac events can occur, including Takotsubo cardiomyopathy. Takotsubo cardiomyopathy, also referred to as stress-induced cardiomyopathy, is an acute, typically reversible myocardial dysfunction syndrome. It is caused by a sudden surge of catecholamines precipitated by a stressor, which can be emotional or physical, that temporarily stuns the heart.
Takotsubo cardiomyopathy can present like acute coronary syndrome (ACS) with an absence of significant coronary artery obstruction. It most commonly occurs in postmenopausal women and may arise after initial or subsequent ECT sessions. While patients most often have a favorable prognosis with eventual normalization of cardiac function, a significant number of patients experience hemodynamic instability, and some patients may experience persistent symptoms. Thus, Takotsubo cardiomyopathy is an important cardiovascular risk to consider prior to initiating ECT therapy. We present a case of ECT-induced Takotsubo cardiomyopathy in a 67-year-old woman, followed by a discussion of peri-procedural cardiac risk assessment and considerations for resumption of ECT therapy after the occurrence of TCM.
While cases of ECT-induced Takotsubo cardiomyopathy have been previously reported, this case is notable for the development of TCM after the first ECT session in a patient with known coronary artery disease and concurrent stimulant therapy, highlighting the potential additive effect of multiple sympathetic stressors. This case underscores the importance of individualized cardiovascular risk assessment and raises considerations for peri-procedural management in higher-risk populations. In addition to postmenopausal women, other populations at increased risk include patients with underlying psychiatric or neurologic illness and those exposed to significant physical or psychological stressors.
Case presentation
A 67-year-old woman with a history of CAD, bipolar disorder, COPD, ADHD, breast cancer in remission, obesity, hyperlipidemia, and remote tobacco use presented with acute onset of chest pain following her first session of electroconvulsive therapy. Her psychiatric history was notable for a one-year course of a worsening depressive episode of bipolar I disorder associated with passive suicidal ideation. She was taking Lurasidone, Adderall, and Lithium, and was enrolled in a psychiatric partial program where she underwent a brief consultation to receive ECT. In terms of cardiac risk factors, she had a long history of tobacco use (approximately one pack per day for several decades) but quit smoking in recent years and denied alcohol use. She was noted to have a history of hyperlipidemia on statin therapy, class I obesity, and CAD incidentally noted on a previous CT chest as moderate coronary artery calcification. She had a prior echocardiogram that showed normal biventricular size and systolic function, without evidence of regional wall motion abnormalities.
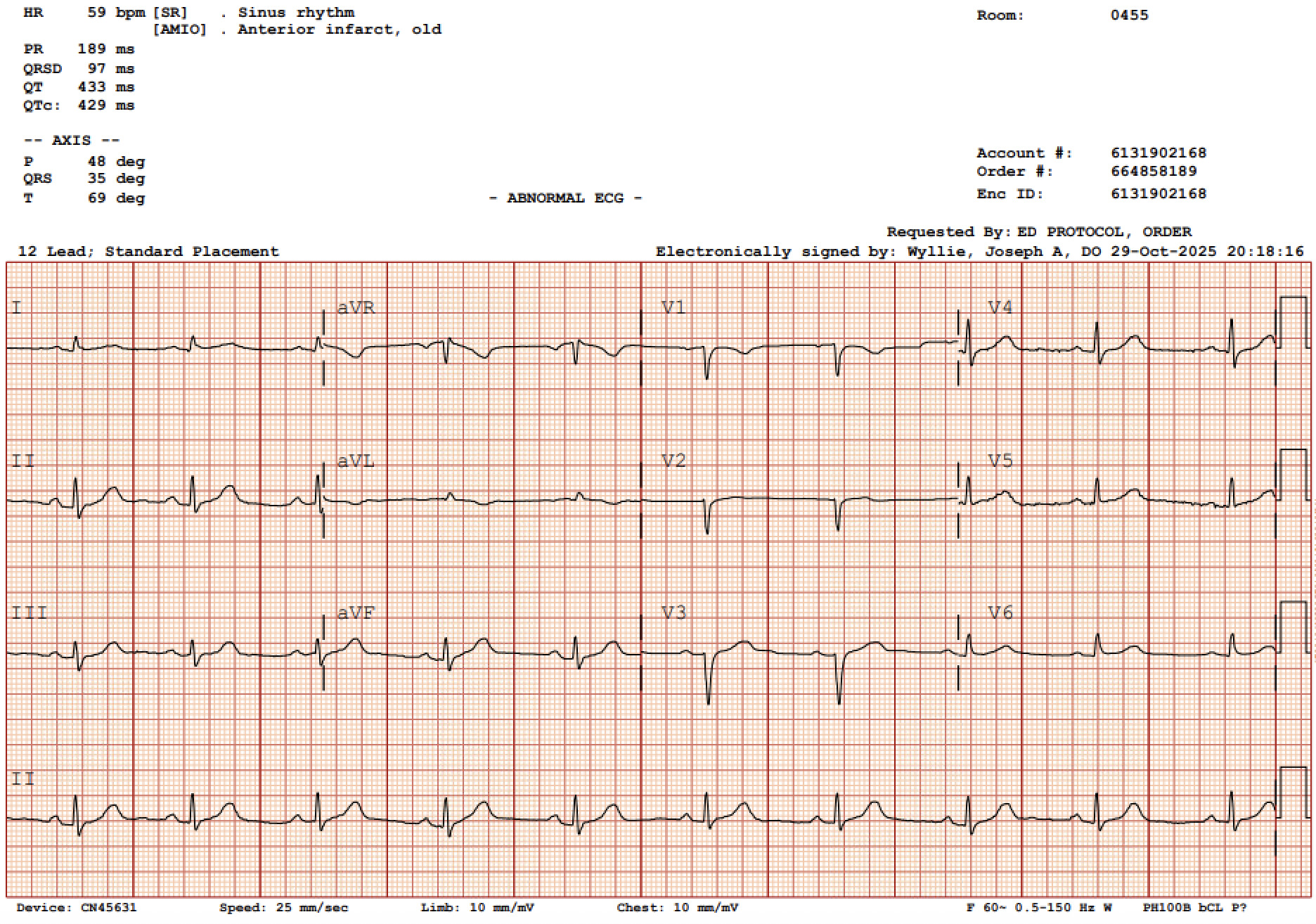
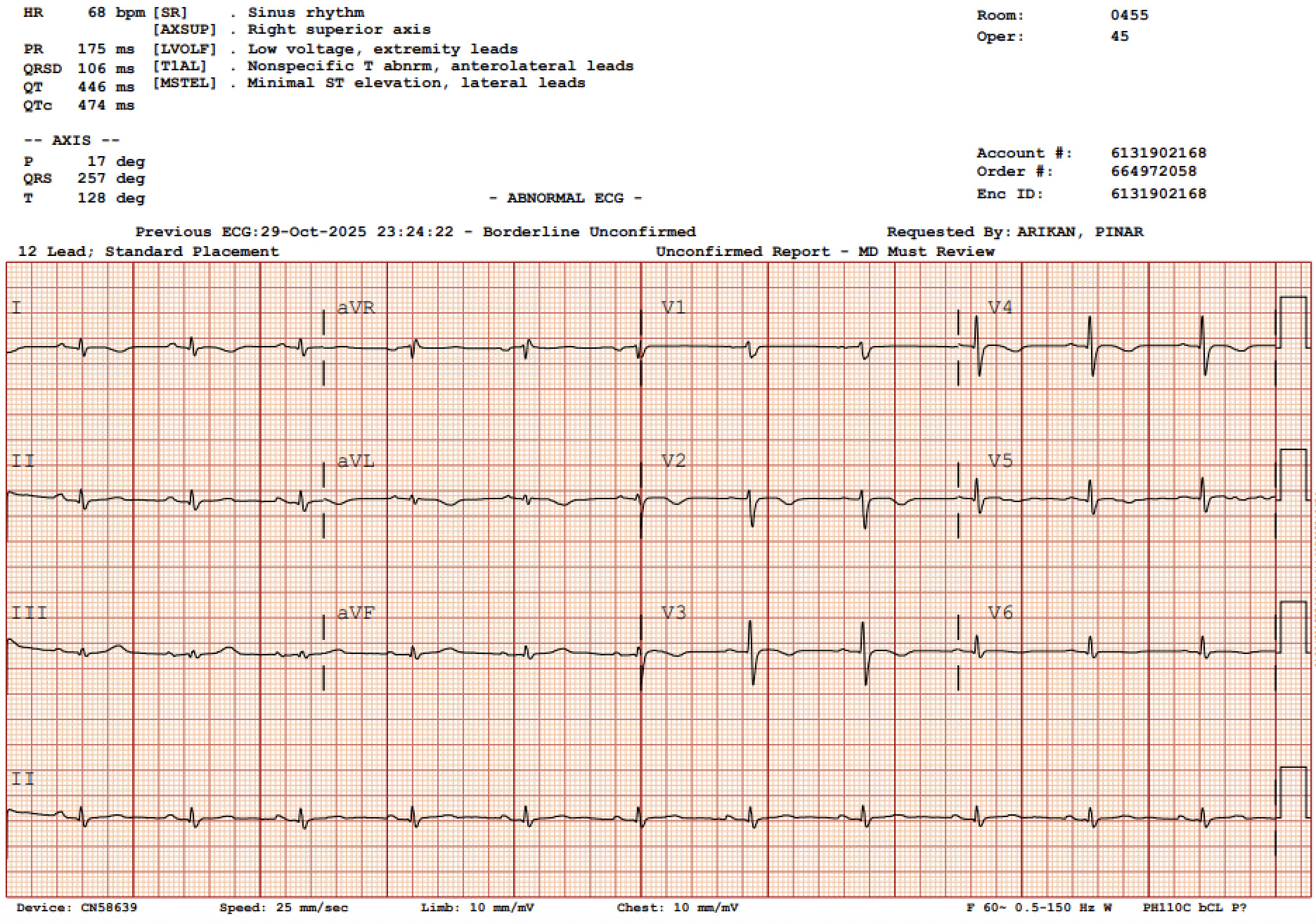
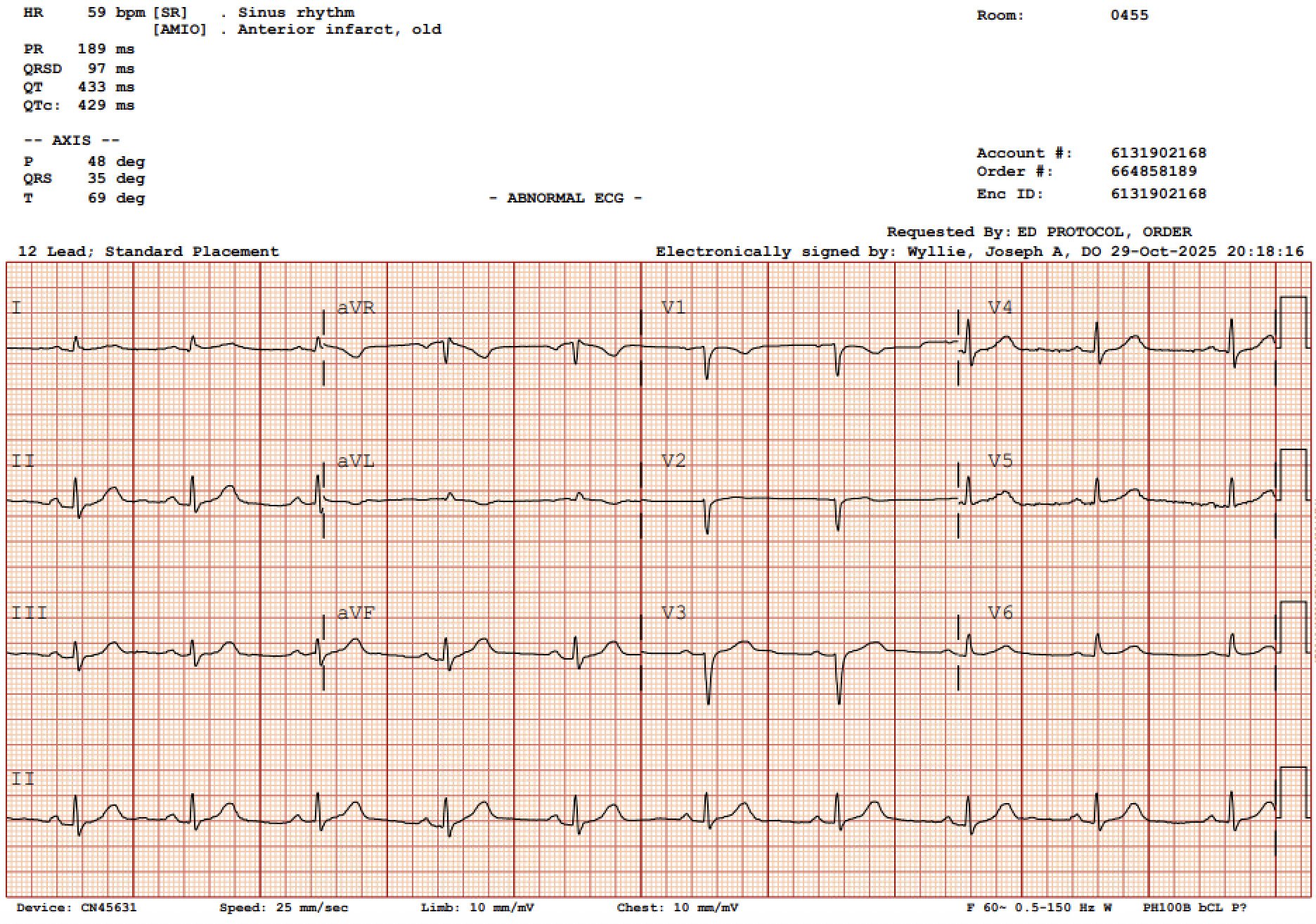
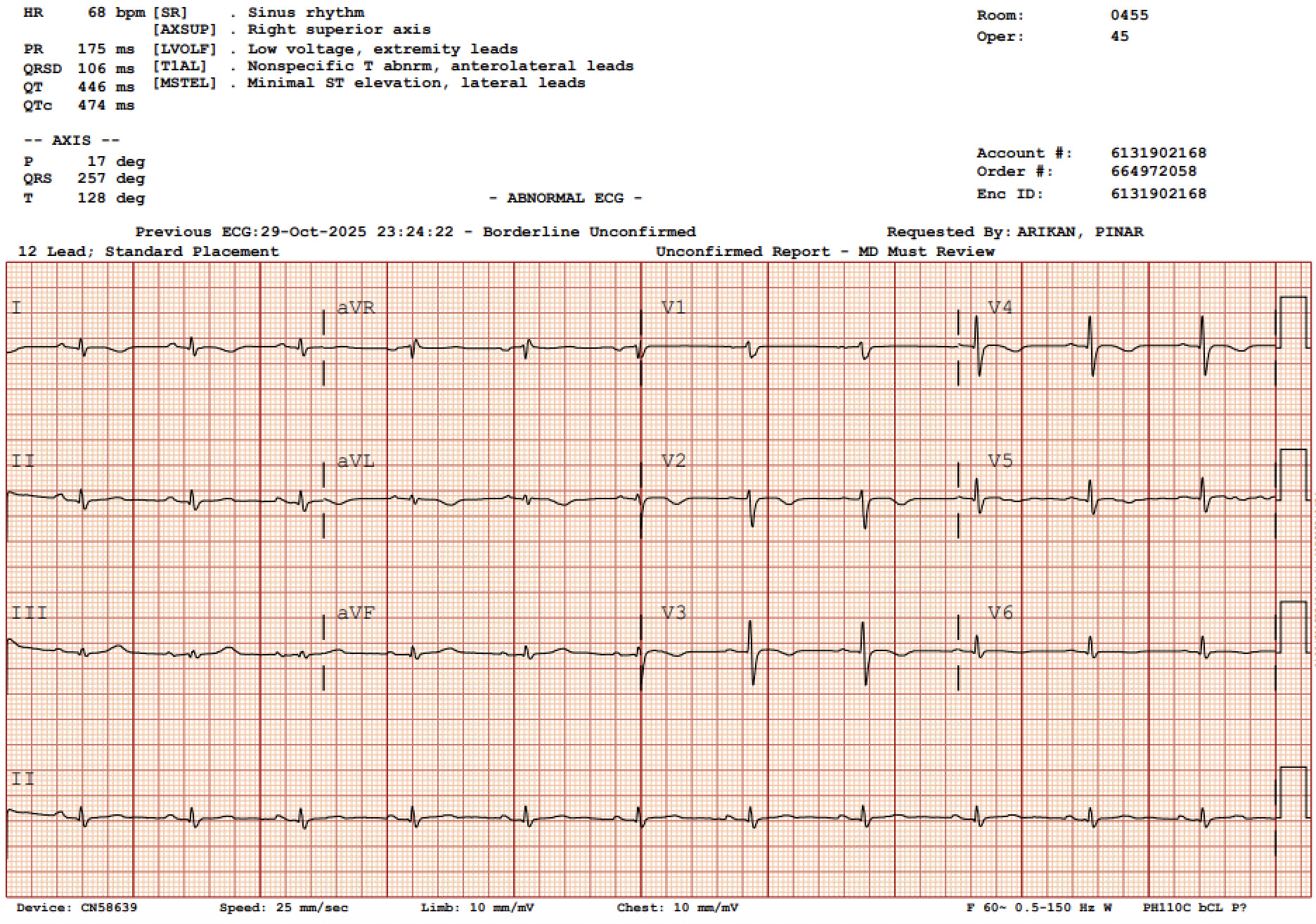
The patient was started on ECT in the outpatient setting. Anesthesia was induced with methohexital and succinylcholine. Bifrontal electrode placement was used, with an initial energy setting of 40%, pulse frequency of 30 Hz, and seizure durations of 18 seconds (observed) and 20 seconds (EEG). The clinical seizure was deemed satisfactory, and the energy level was planned to be increased to 60% for the subsequent session. Approximately four hours after awakening from the ECT procedure, the patient experienced sudden onset of substernal chest discomfort radiating to her left arm. She had no known history of myocardial infarction or prior cardiac intervention. Vital signs were stable. Her high sensitivity troponin level on presentation reached a maximum of 3,185 ng/L. EKG initially demonstrated sinus rhythm with normal intervals (Figure 1). On serial EKGs, acute T wave inversions were notable in the anterolateral leads (Figure 2).
Cardiology was consulted, and the patient underwent coronary angiography, which demonstrated no evidence of coronary obstruction. Transthoracic echocardiogram revealed the left ventricle was mildly dilated with moderate systolic dysfunction with a left ventricular ejection fraction of 36% and akinesis of the mid-to-distal apical segments, consistent with Takotsubo cardiomyopathy. Prior to her hospitalization, she was taking aspirin 81 mg and rosuvastatin 10 mg daily. During this hospitalization, she was started on metoprolol succinate 25 mg daily. She was discharged on hospital day 3 with close cardiology follow-up with plans for a repeat TTE in a few months. The patient did not follow up with cardiology for her scheduled repeat TTE. She continued to receive psychiatric care but did not resume ECT.
Discussion
This case highlights the link between ECT and adverse cardiovascular events such as Takotsubo cardiomyopathy. More importantly, it highlights two clinically relevant considerations: (1) optimal pre-ECT cardiovascular risk assessment in patients with known or suspected coronary artery disease, and (2) the safety and timing of resuming electroconvulsive therapy after the occurrence of Takotsubo cardiomyopathy.
Cardiovascular effects of ECT and pathophysiologic link to Takotsubo cardiomyopathy
The prevailing hypothesis for TCM involves catecholamine-mediated myocardial stunning.2,3 ECT induces a biphasic autonomic response: an initial parasympathetic surge (bradycardia, hypotension) and a subsequent sympathetic surge (tachycardia, hypertension, marked catecholamine release).1 Elevated circulating epinephrine and norepinephrine may result in direct myocardial toxicity via β-adrenergic stimulation and cAMP-mediated calcium overload, coronary microvascular dysfunction or vasospasm, supply–demand mismatch, particularly in patients with underlying coronary disease, or myocardial stunning and contraction band necrosis.1,2 Patients with pre-existing cardiovascular risk factors may be more susceptible. Our patient possessed several risk factors, including postmenopausal status, prior tobacco use, stimulant medication use, and underlying coronary artery disease.
Although acute cardiac complications such as cardiomyopathy, arrhythmias, and cardiogenic shock can occur with Takotsubo cardiomyopathy, ventricular function typically recovers in the majority of patients, often within days to weeks, reflecting the reversible nature of myocardial stunning rather than permanent structural injury.4 Ventricular recovery has also been observed in reported cases of ECT-associated TCM.5 The recurrence risk of TCM is approximately 5–10% over several years.6 Factors associated with recurrence include exposure to emotional or physical stressors, underlying psychiatric or neurologic disease, and individual susceptibility to catecholamine-mediated stress. In the context of ECT, repeated sympathetic activation may represent a potential trigger, although data specific to this population remain limited. Importantly, short-term mortality is not negligible and may approach that of ACS in the acute phase.4
Pre-Procedural Cardiac Risk Assessment
ECT is generally considered a low-mortality procedure, with overall mortality comparable to that of minor surgical procedures under general anesthesia.2 However, cardiovascular complications remain the most common adverse events. ECT commonly produces transient arrhythmias and blood pressure fluctuations. Serious cardiac complications are rare but include myocardial ischemia and stress cardiomyopathy. A focused cardiovascular assessment, including a detailed cardiac history (prior myocardial infarction, coronary artery disease, heart failure symptoms, arrhythmias, syncope, exercise tolerance), medication review, and targeted physical examination, along with a baseline EKG are recommended in patients over 50 years of age or those with known cardiovascular disease prior to ECT initiation. Additional testing, such as echocardiography, stress testing, or cardiology consultation, is reserved for patients with active cardiac symptoms, poor functional capacity (<4 metabolic equivalents of task), decompensated heart failure, significant valvular disease, or other high-risk features.1
This case raises the question of whether additional evaluation should be considered in select high-risk populations - particularly postmenopausal women with known coronary artery disease and atherosclerotic risk factors, as well as those on stimulant class medications. While there is no guideline recommending routine echocardiography or stress testing prior to ECT in asymptomatic patients, clinicians should carefully evaluate cardiac risk factors. In patients with known CAD, even if incidentally detected, shared decision-making with cardiology may be reasonable, especially when additional risk modifiers (e.g., stimulant use, significant anxiety, obesity) are present. Notably, our patient was prescribed amphetamine salts, which may further augment sympathetic tone and could theoretically amplify catecholamine response during ECT, though direct evidence is limited.
Resuming ECT after Takotsubo cardiomyopathy
The question of whether ECT can be restarted after TCM is clinically significant, particularly in patients with severe, treatment-resistant mood disorders where ECT may be life-saving. The development of TCM following ECT is not considered an absolute contraindication to future sessions. Case reports describe successful re-initiation after normalization of left ventricular function, with implementation of cardioprotective strategies.6,7 These include delaying ECT until LVEF normalization, peri-procedural beta-blockade, close hemodynamic monitoring, and ECT intensity adjustments such as decreasing seizure duration.8–10
In particular, beta-blockers may reduce the risk of recurrence by attenuating catecholamine-mediated myocardial stress, though evidence remains inconclusive. In a systematic review of 24 cases of ECT-induced TCM, beta-blockers were the most commonly used preventive measure during ECT retrial. Notably, 8 of 24 cases developed TCM despite prophylactic beta-blocker use during the initial ECT course, suggesting that beta-blockers do not reliably prevent first-occurrence TCM. However, all 8 patients who underwent ECT retrial completed treatment without TCM recurrence. While these findings suggest that beta-blockade may be considered as part of a risk mitigation strategy in patients with prior TCM, the evidence remains limited.5 Alpha-adrenergic modulation has also been hypothesized as protective.11 Particular caution may be warranted in patients with multiple risk modifiers, including established coronary artery disease and stimulant use, as seen in this case.
Risks and benefits must be carefully weighed prior to ECT re-initiation after TCM, as recurrence of TCM after ECT re-initiation has been reported. Formal guidelines are needed to address the resumption of ECT after TCM. Given this patient’s severe refractory depression and chronic suicidal ideation, multidisciplinary, shared decision-making involving psychiatry, cardiology, and anesthesia is essential prior to resuming ECT. The potentially life-saving psychiatric benefit of ECT must be weighed against the low but non-negligible risk of TCM recurrence.
Conclusion
Electroconvulsive therapy-associated Takotsubo cardiomyopathy represents a rare but clinically significant complication driven by catecholamine-mediated myocardial stunning. Although ECT is generally safe and remains a highly effective treatment for severe mood disorders, its predictable sympathetic surge may precipitate transient left ventricular dysfunction in susceptible individuals. Prompt evaluation with cardiac biomarkers, serial electrocardiography, echocardiography, and coronary angiography when indicated is essential to differentiate Takotsubo cardiomyopathy from acute coronary syndrome. Importantly, the development of Takotsubo cardiomyopathy does not constitute an absolute contraindication to further ECT. Following recovery of ventricular function, careful multidisciplinary reassessment, including cardiac optimization and consideration of peri-procedural sympathetic attenuation strategies, may allow safe resumption of therapy when psychiatric benefit outweighs cardiovascular risk. This case reinforces the need for heightened clinical vigilance, interdisciplinary collaboration, and individualized risk stratification when managing patients undergoing ECT, particularly those with baseline cardiovascular comorbidities.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding author
Pinar Arikan MD,
Department of Medicine,
Warren Alpert Medical School of Brown University,
Division of Hospital Medicine, Miriam Hospital,
Providence, RI 02906
Email: parikan@brownhealth.org