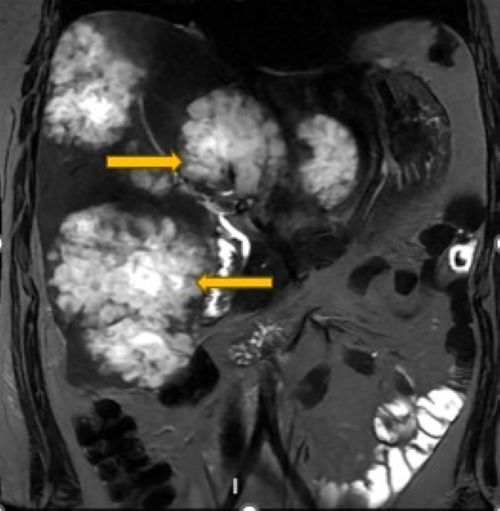
A 34- year- old woman with no significant past medical history presented with progressive right upper quadrant pain, fatigue, and unintentional weight loss of 18 pounds over five months. She denied fever, chills, night sweats, or other signs of infection. The physical exam was unremarkable except for right upper quadrant tenderness. Laboratory tests showed anemia (hemoglobin: 11. 5 g/dL) and elevated liver enzymes (total bilirubin: 0. 0.8 mg/dL, alkaline phosphatase: 475 U/L, aspartate aminotransferase: 94 U/L, and alanine aminotransferase: 74 U/L). Abdominal and pelvic CT revealed 10 cystic liver lesions, the largest measuring 89 x 82 x 94 mm, suspicious for abscesses or metastases. Magnetic resonance imaging of the liver demonstrated multiple large, multilobulated, undulating “cauliflower- like” masses involving the right, left, and caudate lobes. The lesions were predominantly T2 hyperintense with internal hypointense septations, suggesting complex architecture, and appeared hypointense on dual- echo sequences. They exerted significant mass effects, including displacement of the pancreatic body and tail and attenuation of the main and left portal veins. These features were highly suspicious for malignancy (Figure 1). The imaging findings prompted a broad differential diagnosis in a young female.
__t2-_weighted_image_showing_cauliflower-like_hyperinte.jpeg)
Hepatic abscesses were initially considered based on the cystic appearance on CT; however, the absence of systemic infection and the lack of rim enhancement or diffusion restriction made this unlikely. Biliary cystic neoplasms and intraductal papillary neoplasms were less favored, given the absence of ductal dilation or internal projections. Atypical hemangiomas and intrahepatic cholangiocarcinoma were also considered but lacked characteristic enhancement patterns. Overall, the unusual morphology raised a strong suspicion of metastatic disease. Serum tumor markers were elevated: carcinoembryonic antigen: 94 ng/mL, CA 19-9: 6000 U/mL, and CA 125: 55 U/mL. Liver biopsy confirmed metastatic mucinous adenocarcinoma, consistent with colorectal origin. Colonoscopy identified multiple polyps in the sigmoid, transverse, and ascending colon; biopsy confirmed invasive adenocarcinoma arising from a tubulovillous adenoma in the sigmoid colon. The patient was started on palliative chemotherapy after a multidisciplinary discussion. The atypical imaging appearance played a crucial role in guiding management. Given the broad differential diagnosis, tissue biopsy was prioritized to establish a definitive diagnosis before initiating therapy. This approach prevented potential misdiagnosis and ensured the timely initiation of appropriate oncologic treatment.
Metastatic liver lesions are a common site of spread in colorectal cancer, with the liver involved in roughly 25–50% of cases.1 Liver metastases from colon adenocarcinoma typically appear on imaging as round or oval, hypodense masses with a central hypoattenuating area surrounded by a peripheral enhancing rim, known as the “target appearance”.2 However, the cauliflower-like shape of the liver lesions, as seen in this case, posed a diagnostic challenge because of their rarity and unusual form. This uncommon presentation highlights the importance of maintaining a high suspicion for metastatic colorectal cancer, even in younger patients without typical risk factors. The early onset of metastatic colorectal cancer in this patient raises concern for hereditary cancer syndromes, such as Lynch syndrome and familial adenomatous polyposis, particularly given the presence of multiple colonic polyps. Although genetic evaluation was beyond the scope of this report, this case underscores the importance of considering hereditary predisposition and its implications for family screening and surveillance. It also underscores the need for tissue biopsy to confirm the diagnosis, as imaging alone may not always provide a definitive answer, especially when lesions display atypical features. Recognizing rare metastatic patterns early is essential for timely diagnosis and appropriate treatment, particularly in younger individuals.
Disclosures/Conflicts of Interest
The authors disclose no conflicts of interest
Corresponding author
Nidha Shapoo MD,
Department of Medicine, New York Medical College/Metropolitan Hospital,
New York, United States of America.
Email: nidha.shapoo@gmail.com