Background
Infective endocarditis (IE) is associated with a significant inpatient mortality rate, estimated between 15% and 20%.1 During the 1960s, when the condition began to be systematically studied, viridans streptococci was identified as the most common causative organism. However, the epidemiologic profile of IE has since shifted, with Staphylococcus aureus now recognized as the predominant pathogen.1 This change is attributed in part to the increasing prevalence of intravenous drug use in North America, as well as the growing incidence of healthcare-associated infections, which currently account for approximately 30% of all IE cases.2
Optimal management of IE requires pathogen-specific therapy guided by blood cultures and antimicrobial susceptibility testing. The duration of treatment is determined by several factors, including the bactericidal efficacy of the selected antibiotic, the pathogen’s minimum inhibitory concentration (MIC), the burden of vegetation, and the anatomical site of infection; typically, antibiotic therapy ranges from two to six weeks.3 The presence of a bioprosthetic valve or implantable cardiac device substantially influences both the choice and duration of antibiotic treatment.4 These infections are generally more severe and are associated with increased mortality, higher complication rates, and a greater likelihood of treatment failure compared to infections involving native valves, even when the same pathogen is implicated. Furthermore, patients with prosthetic valves or cardiac devices are at heightened risk for developing IE. In such cases, particularly in the setting of prosthetic valve or healthcare-associated endocarditis, empiric antibiotic regimens should provide coverage against methicillin-resistant Staphylococcus aureus (MRSA), enterococci, and gram-negative organisms.4
Methods
This scoping review was completed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) checklist. We searched for English-language published studies classified as clinical trials and randomized control trials in MEDLINE (up to December 31, 2025), discovered through multiple search queries specifying for “infective endocarditis” or “endocarditis” and specific drug classes (including “penicillin,” “aminoglycosides,” “vancomycin,” “cephalosporins,” “rifampin,” “daptomycin,” “fluoroquinolones,” and “antimicrobials” to capture remaining studies not discovered by searches specifying drug classes).
Diagnostic criteria
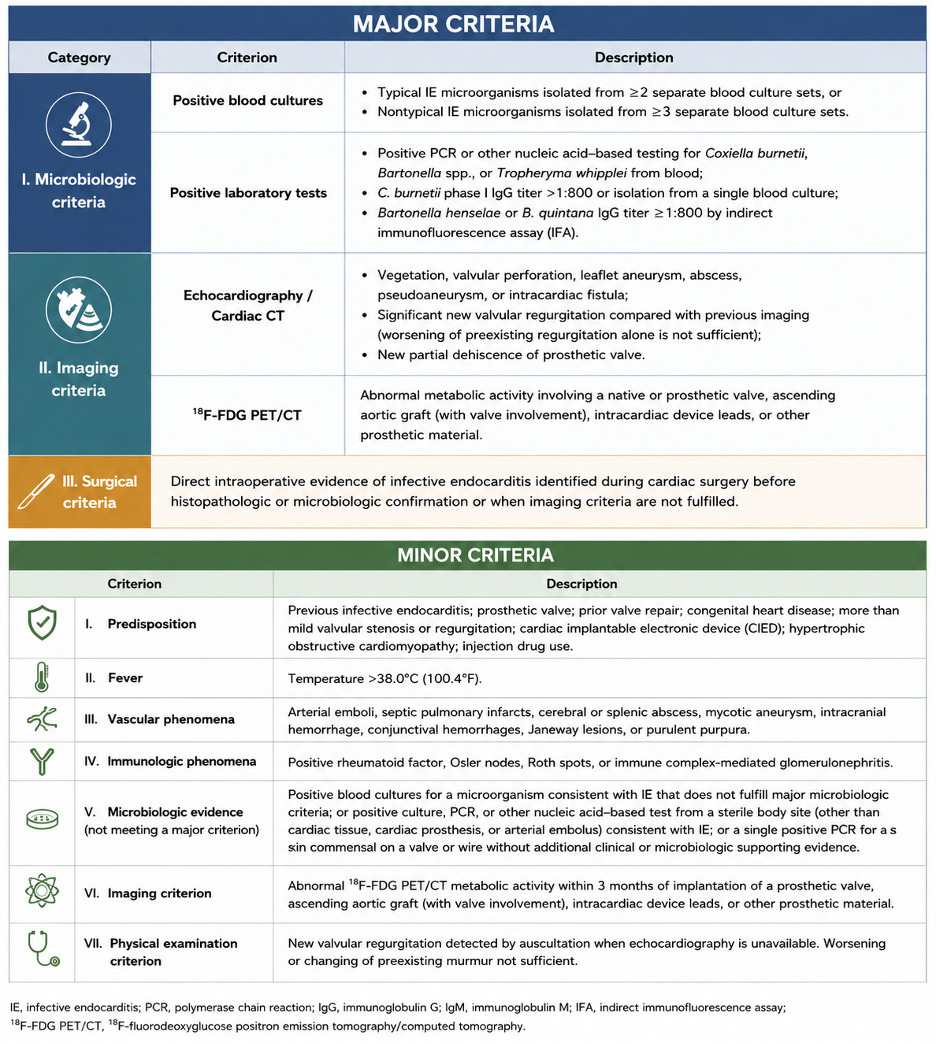
Table 1 presents the updated diagnostic categories for infective endocarditis (IE) using the 2023 Duke–ISCVID criteria.5 It explains how a case is classified as definite, possible, or rejected by combining clinical, microbiological, imaging, and pathological evidence. A diagnosis of definite IE can be established by pathological confirmation or by fulfilling a combination of clinical criteria (such as multiple major or major plus minor findings). Possible IE is applied when there is supportive but incomplete evidence, such as fewer criteria being met. The rejected category applies when an alternative diagnosis is more likely, when the illness resolves quickly with a short course of antibiotics, or when pathological examination fails to demonstrate evidence of infection. The major criteria include the most specific findings, such as persistently positive blood cultures for typical organisms, imaging evidence of endocardial involvement (vegetations, abscesses, or prosthetic valve dehiscence), and new valvular regurgitation. The minor criteria represent supportive findings that increase the likelihood of IE but are not individually diagnostic, including predisposing conditions (such as IV drug use or structural heart disease), fever, vascular and immunologic phenomena, and microbiological evidence that does not meet the major thresholds.5 (Figure 1)

Epidemiology
Left-sided infective endocarditis (LSIE) is more common, typically affects older patients, and is often associated with underlying structural heart disease or prosthetic valves. The most common pathogens are streptococcal and staphylococcal species. Clinical features often include systemic embolic phenomena, immunologic manifestations, and heart failure due to valvular destruction. Complications such as paravalvular abscesses and invasive disease are more frequent and severe in left-sided disease. Mortality is higher compared to right-sided disease.6
Right-sided infective endocarditis (RSIE) accounts for 5–10% of all cases of IE.6 It is most commonly seen in younger patients, especially those with intravenous drug use, indwelling catheters, pacemakers, or congenital heart disease. Staphylococcus aureus is the predominant pathogen in IV drug users, whereas viridans streptococci is predominant in non-IV drug users.7 Clinical presentation is often characterized by persistent fever and respiratory symptoms due to septic pulmonary emboli, while systemic embolic and immunologic phenomena are less common. Right-sided endocarditis is less likely to be invasive or cause paravalvular abscesses and generally has a more favorable prognosis, with lower mortality and higher cure rates, especially in uncomplicated cases.6,7 In pediatric patients risk factors (e.g., congenital heart disease), and management considerations differ and are summarized in the AHA pediatric update.8 The scope of this review is largely limited to the management of LSIE.
Native Valve Endocarditis
Native valve endocarditis (NVE) remains a significant clinical challenge, necessitating timely recognition, microbiological diagnosis, and appropriate antimicrobial therapy. The treatment approach is determined by the causative organism, its resistance profile, and patient-specific factors, including drug allergies and comorbidities.9 Table 2 summarizes the treatment recommendations for NVE.3
In streptococcal NVE, the penicillin MIC is important. For isolates with a penicillin MIC ≤0.12 µg/mL, treatment with intravenous penicillin G or ceftriaxone for 4 weeks is recommended.3 In select, uncomplicated cases, a shortened 2-week regimen of penicillin G or ceftriaxone in combination with gentamicin may be considered, provided the patient demonstrates a prompt clinical response and has no underlying renal impairment. For isolates with relatively reduced penicillin sensitivity (MIC >0.12-<0.5 µg/mL), combination therapy with penicillin G or ceftriaxone plus gentamicin is recommended. In patients with a β-lactam allergy, vancomycin administered for 4 weeks is an appropriate alternative; in this setting, the addition of gentamicin is not necessary.3 In select cases, step-down therapy to oral amoxicillin may be considered once adequate control with intravenous treatment has been established.10 For isolates with a penicillin MIC >0.5 µg/mL, treatment should consist of a combination regimen similar to that recommended for enterococcal NVE. Higher doses of intravenous penicillin are recommended than those used for fully susceptible strains.3
For Staphylococcus aureus NVE, methicillin susceptibility is a critical determinant of therapy. For methicillin-susceptible Staphylococcus aureus (MSSA), the first-line treatment is intravenous nafcillin or oxacillin for 6 weeks. Intravenous cefazolin for 6 weeks is an alternative for patients with non-anaphylactoid penicillin allergy. For MRSA NVE, the recommended agents are intravenous vancomycin or daptomycin for 6 weeks.3
Enterococcal NVE presents additional complexity due to intrinsic and acquired resistance. Effective regimens rely on synergistic combinations. Typically, ampicillin plus gentamicin, ampicillin and ceftriaxone, penicillin plus gentamicin, or, in some cases, vancomycin plus gentamicin.11 In vancomycin-resistant strains, alternatives such as daptomycin or linezolid must be considered.11 Gram-negative bacilli, although less frequent, pose a therapeutic challenge due to their high mortality rates and multidrug resistance.12 HACEK organisms remain reliably susceptible to ceftriaxone and fluoroquinolones, whereas non-HACEK gram-negative bacilli require prolonged combination therapy and are often associated with poor outcomes.3
A universal principle across all regimens is the use of prolonged intravenous therapy, generally lasting 4–6 weeks, reflecting the difficulty of sterilizing infected cardiac valves. Adjunctive measures, including repeat blood cultures and early surgical evaluation in cases of persistent infection, heart failure, or embolic complications, remain essential for optimizing outcomes.3 Persistent infection is defined as positive blood cultures beyond 48–72 hours of appropriate therapy, or infection due to fungi and highly resistant organisms. In cases of persistent MSSA bacteremia beyond 72 hours, it may be reasonable to consider initiating dual β-lactam therapy. The combination of ertapenem and cefazolin for treating persistent MSSA bacteremia, particularly in the context of infective endocarditis, was first described in 2016.13 Since then, several case reports and meta-analyses have examined the efficacy of this dual-antibiotic regimen. While a recent meta-analysis did not demonstrate a significant difference between monotherapy and combination therapy in terms of time to blood culture clearance or 90-day mortality, the data remain limited.14,15
Prosthetic Valve Endocarditis
Prosthetic Valve Endocarditis (PVE) represents one of the most severe forms of infective endocarditis, requiring both timely diagnosis and carefully selected antimicrobial therapy. Early PVE typically results from direct intraoperative contamination or hematogenous seeding of the prosthetic valve within the initial days to weeks following surgery.16 Paravalvular abscess formation is a common complication associated with both mechanical and bioprosthetic valves. Between two and twelve months postoperatively, PVE is generally attributed to either late-onset nosocomial infection or community-acquired sources.16 Table 3 summarizes the treatment recommendations for PVE.3
During the first two months after valve implantation, Staphylococcus aureus is the most frequently isolated pathogen, followed by coagulase-negative staphylococci, gram-negative bacilli, and candida species.18 Infections occurring between two and twelve months are most commonly caused by streptococcus species, Staphylococcus aureus, and coagulase-negative staphylococci, with Staphylococcus epidermidis being the predominant coagulase-negative species, typically demonstrating methicillin susceptibility.18,19 Enterococcal species are also frequently implicated during this period.11 Late-onset PVE, defined as infection occurring more than twelve months postoperatively, is usually secondary to community-acquired bacteremia. The microbial spectrum closely resembles that of native valve endocarditis, with streptococcus species, Staphylococcus aureus, coagulase-negative staphylococci, and enterococcus species being the most common etiologic agents.19 Empiric regimens differ by timing of onset: early PVE (≤1 year post-surgery) requires treatment with vancomycin, gentamicin, rifampin, and cefepime to account for Staphylococci (including MRSA), enterococci, and gram-negative bacilli.19,20 Late PVE (>1 year) narrows empiric therapy to vancomycin plus ceftriaxone, reflecting the predominance of staphylococci, viridans group streptococci, enterococci, and HACEK organisms.19,20
Once the causative pathogen is identified, therapy is tailored. Staphylococcal PVE requires triple therapy, either nafcillin/oxacillin, gentamicin, and rifampin in methicillin-susceptible cases, or vancomycin-based regimens in methicillin-resistant cases.3,21 If coagulase-negative staphylococci are resistant to gentamicin, an alternative aminoglycoside or a fluoroquinolone may be considered if the isolate is susceptible. The treatment for streptococcal PVE (caused by viridans group streptococci or Streptococcus gallolyticus) is 6 weeks of either aqueous crystalline penicillin G, ampicillin, or ceftriaxone, with or without gentamicin for the first 2 weeks if the strain is highly penicillin-susceptible (MIC ≤0.12 µg/mL).3,22 For strains with a penicillin MIC >0.12 µg/mL, a combination of penicillin, ampicillin, or ceftriaxone plus gentamicin for the full 6 weeks is reasonable.3,22 Vancomycin is reserved for patients unable to tolerate penicillin, ceftriaxone, or gentamicin. Enterococcal PVE necessitates synergistic combinations such as ampicillin with gentamicin or ceftriaxone, while vancomycin or daptomycin is reserved for resistant strains.3,16
Culture-negative endocarditis may present early, often reflecting acute and aggressive pathogens such as S. aureus, Gram-negative bacilli, or fungi, or late, typically involving more indolent organisms, including nutritionally variant streptococci, HACEK organisms, or other fastidious pathogens.3,16 Early culture-negative PVE (£1 year after valve replacement) warrants broad empiric coverage for MRSA, resistant Gram-negative organisms, and difficult-to-treat pathogens using a combination of vancomycin, cefepime, rifampin, and gentamicin, whereas late culture-negative PVE (>1 year after valve replacement) is best treated with vancomycin plus ceftriaxone to target streptococci, enterococci, and HACEK species.3 Both native and prosthetic valve culture-negative endocarditis requires at least six weeks of antimicrobial therapy, reflecting the difficulty in eradicating infection when no pathogen is identified. Because prosthetic valve endocarditis carries higher relapse and mortality rates, early surgical intervention is often necessary, particularly in the presence of hemodynamic compromise, prosthetic dysfunction, uncontrolled infection, or elevated embolic risk.16
The use of rifampin in the management of prosthetic valve endocarditis is primarily reserved for staphylococcal infections, including both Staphylococcus aureus and coagulase-negative staphylococci, owing to its unique activity against biofilm-associated organisms and its ability to penetrate prosthetic material.21,23,24 In contrast, rifampin is not routinely recommended for prosthetic valve endocarditis caused by non-staphylococcal pathogens, such as streptococci or enterococci. Rifampin should not be used as monotherapy, and its initiation timing requires careful consideration.21,23,24 Susceptibility testing of the isolate should be performed before initiation of treatment to help reduce the risk of resistance. Gentamicin is often incorporated to provide synergistic bactericidal activity in combination with cell wall–active agents such as beta-lactams or vancomycin. Its role is crucial in enhancing the clearance of organisms embedded within biofilms on prosthetic materials and in reducing the risk of relapse in these challenging infections. Nonetheless, its use is generally dependent on the organism type.3,16,21
Across all scenarios, treatment duration is prolonged, with a minimum of six weeks of intravenous therapy, reflecting the challenges of eradicating infection on prosthetic material.3 The American Heart Association and Infectious Diseases Society of America recommend rifampin for a minimum of 6 weeks, with gentamicin limited to the first 2 weeks of therapy. Although guidelines recommend rifampin- and gentamicin-based regimens for staphylococcal PVE, emerging evidence calls their benefit into question.21 A large Veterans Health Administration cohort found no association between the use of rifampin or gentamicin and improved outcomes.25 Similarly, a European multicenter cohort showed no difference in one-year survival or relapse between rifampin-treated and untreated patients.26 Finally, a systematic review and meta-analysis found no reduction in clinical failure or relapse with either drug, while highlighting risks of hepatotoxicity, nephrotoxicity, and drug interactions.21 All organisms from relapsed cases should be retested for antibiotic susceptibility to guide therapy. Note that studies that evaluated the benefits of synergy between rifampin and gentamicin only evaluated Staphylococcus PVE and not enterococci and other organisms.
Finally, fungal infective endocarditis, whether involving native or prosthetic valves, requires aggressive antifungal therapy and often necessitates surgical intervention due to its high morbidity and mortality. Initial treatment typically consists of lipid-formulation amphotericin B (3–5 mg/kg daily) with or without flucytosine, or a high-dose echinocandin such as caspofungin, micafungin, or anidulafungin.27 Once patients demonstrate clinical stability and clearance of Candida from the bloodstream, step-down therapy with fluconazole (400–800 mg daily) is recommended for susceptible isolates, while voriconazole or posaconazole may be used for fluconazole-resistant species. Surgical intervention is strongly recommended, with antifungal therapy continued for at least six weeks postoperatively and longer when complications such as perivalvular abscess are present. For patients who are not surgical candidates, long-term suppressive therapy with fluconazole is advised to reduce the risk of recurrence, and the same treatment principles apply to both native and prosthetic valve disease.27
Complications and surgical indications
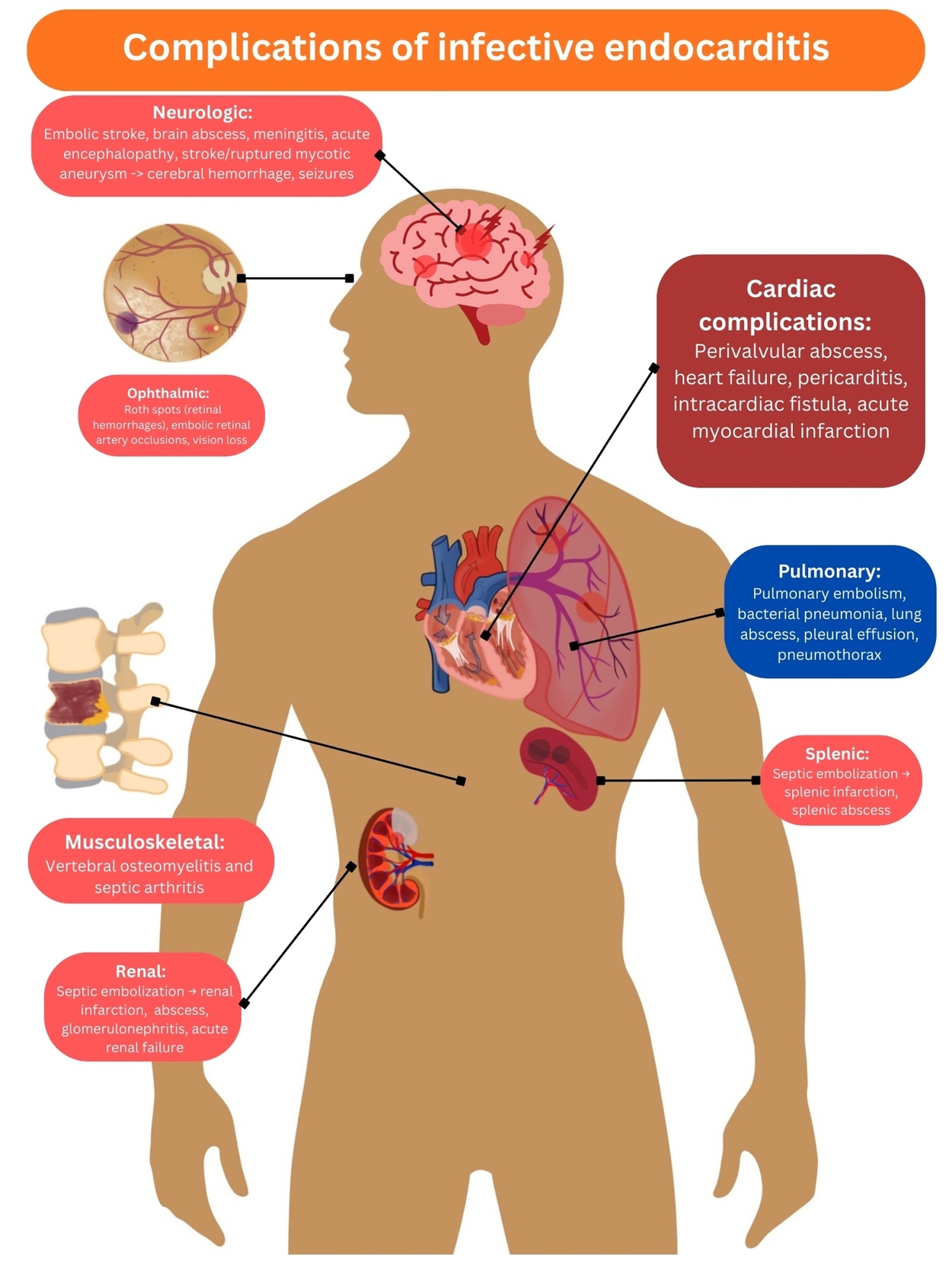
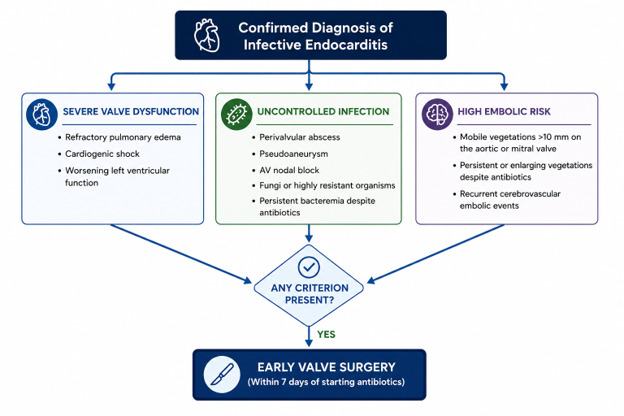
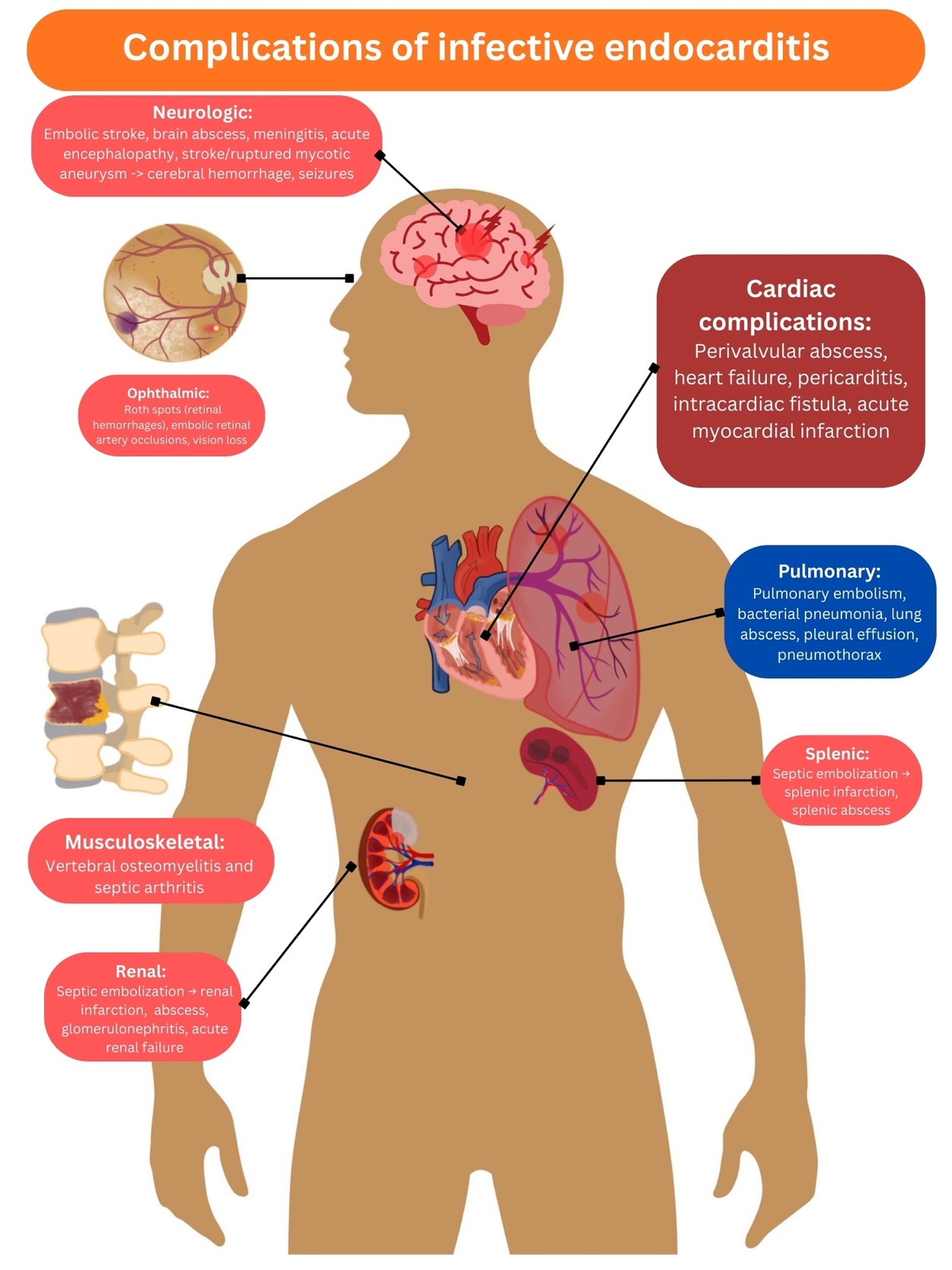
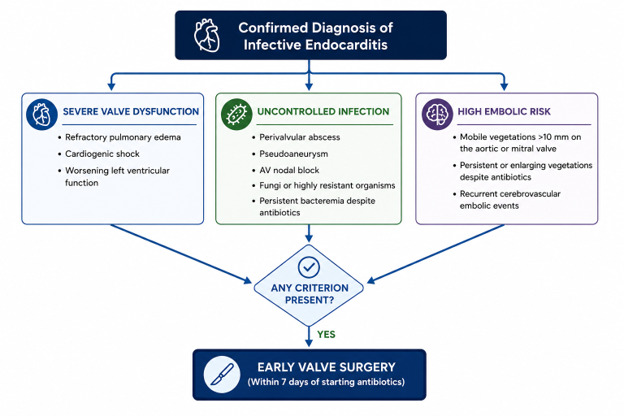
Figure 2 broadly lists the various complications of infective endocarditis. According to the European Society of Cardiology (ESC), surgical intervention for infective endocarditis (IE), whether native or prosthetic valve, is primarily indicated for life-threatening complications such as heart failure, uncontrolled infection, embolic risk, or evidence of local extension.17 Figure 3 lists the indications for early cardiac surgery according to the ESC guidelines.17 Concomitant heart failure, particularly refractory pulmonary edema, worsening left ventricular dysfunction, or cardiogenic shock, remains the strongest predictor of poor prognosis and the most frequent indication for urgent surgery, even before completion of antibiotic therapy.28–30 In addition, locally uncontrolled infection, manifesting as perivalvular abscess, fistula, pseudoaneurysm, or atrioventricular block, represents a critical trigger for expedited operative management.16,31,32 While right-sided IE typically responds to medical therapy, surgery is indicated for patients with severe tricuspid regurgitation causing right-sided heart failure, large vegetations ≥20 mm, and recurrent septic pulmonary emboli despite appropriate antimicrobial treatment, and the American Association for Thoracic Surgery (AATS) recommends applying the same surgical criteria to people who inject drugs despite higher early postoperative risk.3,16,31,33 Certain patients with right-sided infective endocarditis with persistent bacteremia may be considered for vegectomy by interventional cardiology or radiology.34
For prosthetic valve endocarditis, the principles are similar to those for native disease. The most common cardiac complication of PVE is heart failure. This can result from prosthetic valve dehiscence, leading to valvular insufficiency or myocardial infarction due to emboli. Although one study found early surgery in prosthetic valve endocarditis was not associated with lower overall mortality, it was beneficial in patients with strong surgical indications such as severe prosthetic regurgitation, heart failure, paravalvular abscess, fistula, or valve dehiscence.17,31 Other cardiac complications are perivalvular abscess formation, intracardiac fistula, and pericarditis. Ultimately, surgical decisions should be individualized, weighing hemodynamic status, control of infection, neurologic risk, and operative risk.
Non-cardiac complications are usually a result of an embolic event, metastatic abscess formation, or a mycotic aneurysm. Neurologic embolic events occur most frequently in the first days after initiation of antibiotics and decrease significantly after two weeks. Neurologic complications include stroke (due to an embolus), seizure (abscess or emboli), brain abscess formation, aseptic meningitis, acute encephalopathy, cerebral hemorrhage due to ruptured mycotic aneurysm, or meningoencephalitis.35 The timing of surgery depends on vegetation size, mobility, and prior embolic history; current European guidelines recommend early surgery for recurrent emboli, persistent or enlarging vegetations, or vegetations larger than 10 mm, even in the absence of prior embolic events.16 A randomized trial by Kang et al. demonstrated that early surgery (within 48 hours) in native valve endocarditis with large vegetations and severe dysfunction significantly reduced death and embolic events.36 Timing is more complex after neurologic complications: surgery is generally delayed four weeks after intracerebral hemorrhage, but expedited in cases of transient ischemic attack, silent embolism, or ischemic stroke with concurrent surgical indications if hemorrhage is excluded.16
Renal complications include renal infarction due to emboli, renal abscess, glomerulonephritis (resulting from the deposition of immunoglobulins and complement in the glomerular membrane), and acute interstitial nephritis.37 All these complications may present as acute renal failure. Pulmonary complications occur due to right heart PVE; vegetations of the tricuspid or pulmonary valve can lead to embolization, which results in lung abscess, pneumonia, pleural effusion, or pneumothorax.16,33 Other complications are osteomyelitis, septic arthritis, persistent bacteremia, or candidemia in fungal PVE.31 Mortality remains a serious concern after PVE despite appropriate treatment and surgical interventions.16,30,38
Conclusion
The management of infective endocarditis remains a complex and multifaceted clinical challenge that demands a multidisciplinary, multimodal approach. Prolonged courses of intravenous antimicrobial therapy are frequently necessary; however, in specific populations, such as individuals who are incarcerated or who are actively using intravenous drugs, long-term intravenous access or surgical intervention presents unique challenges. Likewise, patients with culture-negative endocarditis or prosthetic valve endocarditis may require advanced diagnostic modalities, including metagenomic next-generation sequencing, 18F-FDG PET/CT, and Cardiac MRI, when clinical suspicion remains high in the absence of evidence of vegetation(s) on echocardiographic studies.16 Optimal outcomes are often achieved through close collaboration among hospitalists, cardiologists, primary care practitioners, infectious disease specialists, addiction medicine specialists, and cardiothoracic surgery specialists. Ongoing vigilance for early complications is essential, as prompt recognition and management are critical to minimizing morbidity and mortality.