A 48-year-old male was diagnosed with left femoral epithelioid vascular neoplasm (favoring epithelioid hemangioendothelioma) on biopsy obtained after imaging detected a suspicious lesion in the context of subacute-on-chronic left lateral knee pain. The patient subsequently underwent left distal femur replacement and surgical resection of the tumor. During routine post-operative care, he developed acute dyspnea and tachycardia. Computed tomography angiography of the chest demonstrated multiple bilateral segmental pulmonary emboli (PE). His transthoracic echocardiogram demonstrated normal left ventricular size, mild concentric thickening, hyperdynamic left ventricular systolic function with ejection fraction >75%, moderate right ventricular enlargement with mildly reduced right ventricular systolic function, an estimated pulmonary artery systolic pressure of 63 mm Hg, and right atrial pressure of 8 mm Hg. Our institution’s PE Response Team was activated in light of these findings; he was placed on anticoagulation and transferred to the intensive care unit for close monitoring.
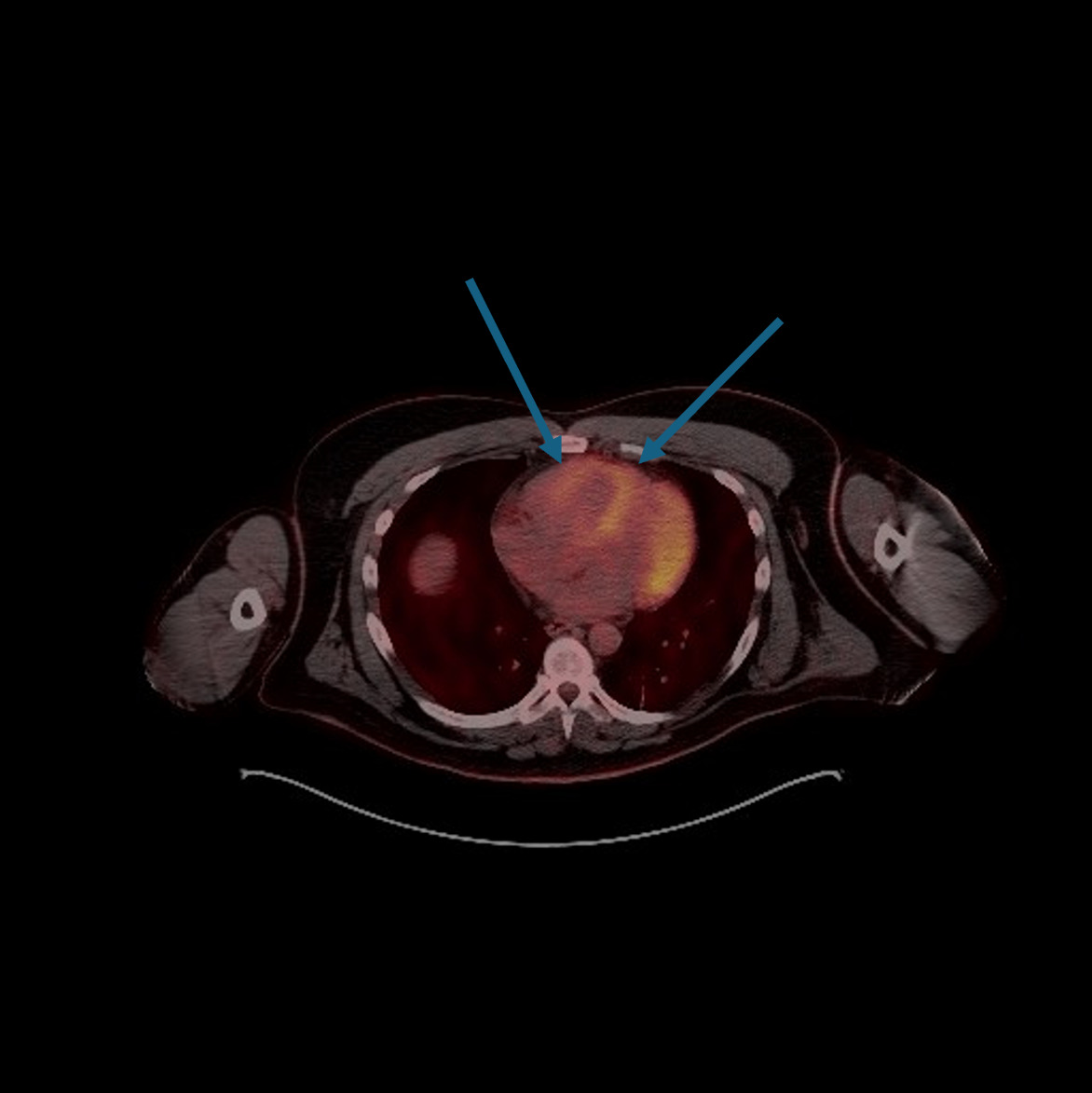
He was hemodynamically stabilized and underwent a previously scheduled Positron Emission Tomography/Computerized Tomography (PET/CT) scan to assess for potential metastatic disease (Figure 1). His remaining femoral space showed no foci of abnormal fluorine-18 fluorodeoxyglucose (FDG) uptake, but the scan incidentally showed FDG uptake in the right ventricular myocardium and left ventricle (LV) as well as main pulmonary artery dilation to 3.4 cm. The histologic features of his malignancy on initial biopsy demonstrated a low mitotic rate, which typically has low FDG uptake; therefore, the absence of corresponding findings on PET/CT did not rule out metastatic disease. Hematology-oncology planned to follow up his post-resection biopsy as an outpatient to determine his treatment plan, and he was discharged on apixaban for an initial duration of six months with the possibility of extending the duration if found to have active metastatic disease on later evaluations.
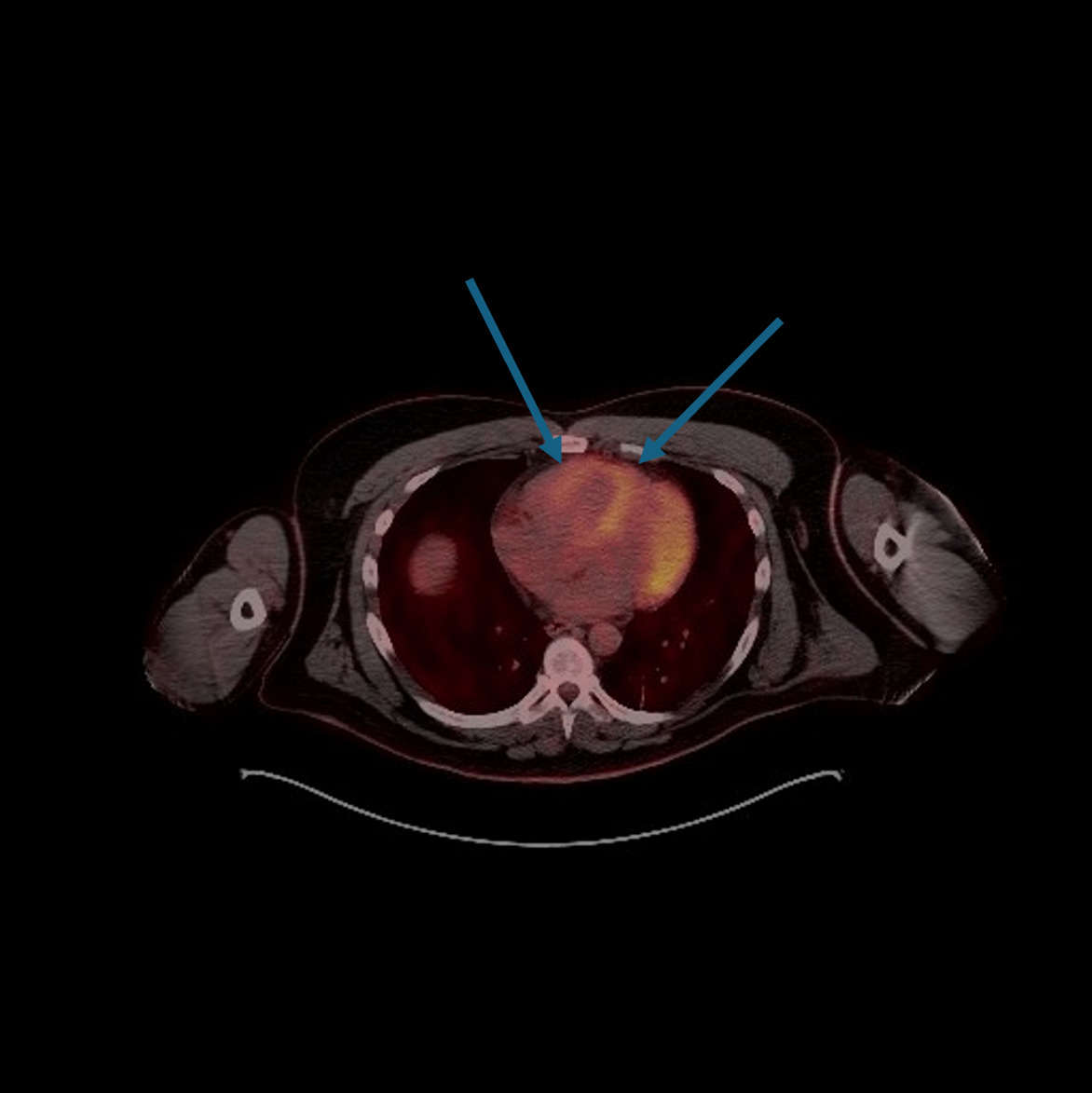
Increased right ventricular FDG uptake is uncommon in patients with PE (reported in only 1.7% of patients) and is more common in patients with pulmonary hypertension.1 Pulmonary hypertension (which leads to right ventricular strain) is more strongly linked to right ventricular FDG uptake and is thought to be related to increased myocardial metabolic demand secondary to pressure overload and elevated right ventricular workload, as well as increased pulmonary angiogenesis, leading to increased metabolic activity.2 In this case, it is unclear if the increased FDG uptake in the LV was related to overall global cardiac metabolic stress from the PE; however, the literature does suggest that the LV may show significant uptake under normal fasting conditions.3 While increased FDG uptake is more commonly seen in chronic causes of pulmonary hypertension, the incidence of acute PE causing this finding is unclear in the literature.4 Recognition of this imaging pattern is important in oncology patients undergoing PET/CT because RV uptake may be misinterpreted as malignant cardiac involvement.
Conflicts of Interest/Disclosures
None
Corresponding author
Satya Patel, MD, FACP
Associate Clinical Professor, David Geffen School of Medicine at University of California, Los Angeles
Hospitalist, Greater Los Angeles Veterans Affairs Healthcare System
11301 Wilshire Blvd Bld 500 Mail Code 111 Los Angeles, CA 90073
Telephone: 310-478-3711 ext 44680
E-mail: satya.patel2@va.gov