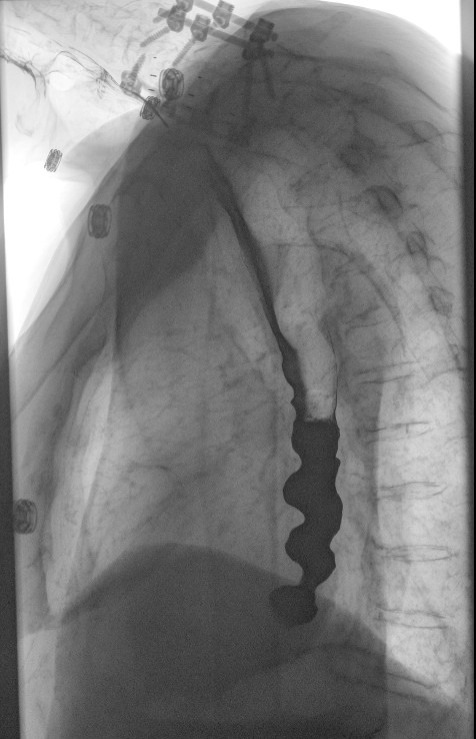
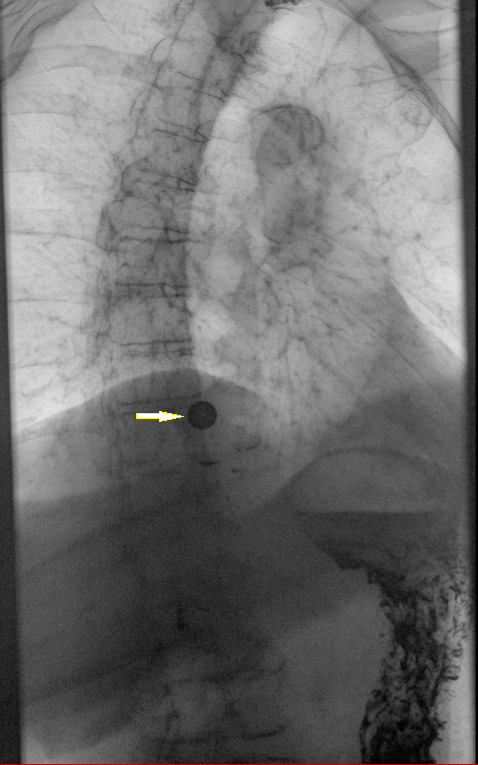

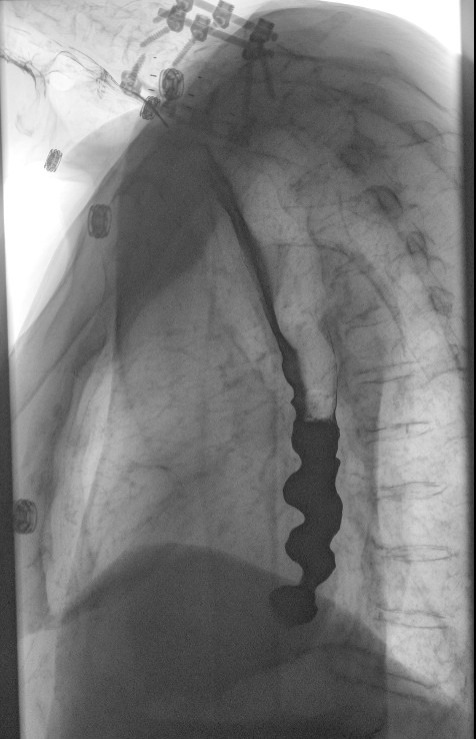
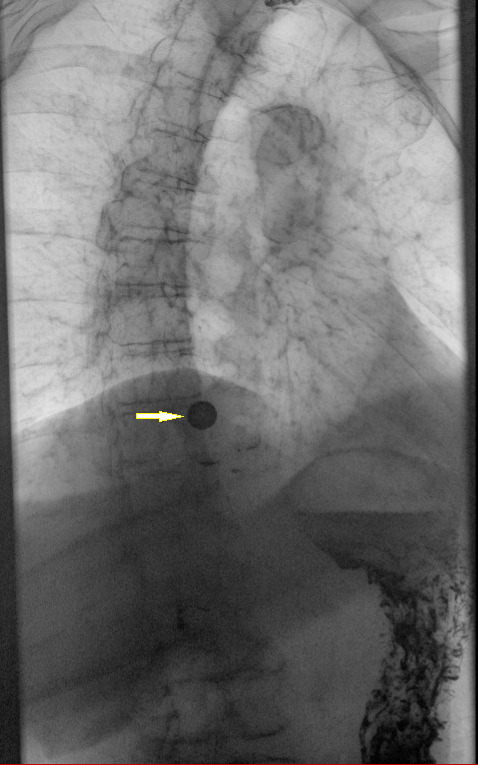
A 77-year-old woman with a history of chronic kidney disease, diabetes mellitus, fibromyalgia, and hypertension presented with one week of dysphagia, regurgitation, and recurrent vomiting. She described a sensation of food “sticking” in the chest, followed by repeated attempts to clear it, resulting in emesis. Symptoms involved both solids and liquids. She denied weight loss, hematemesis, melena, fever, and prior known esophageal disease. Upper endoscopy demonstrated abnormal motility in the lower third of the esophagus without a structural obstruction. The stomach and duodenum were normal. Because symptoms persisted despite the absence of a clear obstructing lesion, a double-contrast fluoroscopic barium esophagram with tablet was performed. This demonstrated a “nutcracker” appearance of the distal esophagus. A barium tablet cleared through the segment without obstruction, and esophageal peristalsis was preserved without the erratic contractions typically seen in distal esophageal spasm (Figures 1–3). The term “nutcracker appearance” in this report is used solely to describe the radiographic morphology observed on barium esophagram and should not be interpreted as a definitive manometric diagnosis. Because the imaging findings suggested an underlying esophageal motility disorder, the patient was referred for outpatient high-resolution manometry for definitive characterization. HRM had not been performed at the time of this report. The patient was discharged on nifedipine and pantoprazole with outpatient gastroenterology follow-up. At follow-up, she reported improvement in dysphagia and regurgitation symptoms.

Hypercontractile esophagus is uncommon, accounting for approximately 1%–3% of high-resolution manometry diagnoses, and is reported more frequently in middle-aged and older adults, particularly women, presenting with dysphagia, regurgitation, or noncardiac chest pain.1,2 The historical term “nutcracker esophagus” has largely been replaced by hypercontractile (jackhammer) esophagus in the era of high-resolution manometry and the Chicago Classification. Associated conditions and proposed risk factors include gastroesophageal reflux disease, esophagogastric junction outflow obstruction, and chronic opioid use, all of which may contribute to abnormal esophageal contractility.1,2 Patients may also report intermittent food impaction, vomiting, or a sensation of food sticking in the chest, with symptoms often fluctuating and nonspecific, contributing to delayed recognition and diagnosis.1,2 Evaluation typically begins with upper endoscopy, followed by esophageal physiology testing when structural or mucosal causes have been excluded.1,2 High-resolution manometry interpreted using the Chicago Classification version 4.0 remains the gold standard for diagnosis and provides a standardized framework for classification of esophageal motor disorders.3–5
Barium esophagram plays an important complementary role in this setting. It may identify structural lesions and provide functional insight into motility disorders, although its sensitivity is limited and findings are not definitive.1,5 A corkscrew or segmented appearance of the distal esophagus is classically associated with distal esophageal spasm, reflecting repetitive nonpropulsive contractions.6 However, similar radiographic patterns may also be seen in a hypercontractile esophagus, highlighting overlap between spastic and hypercontractile disorders on imaging.3,6
Hypercontractile esophagus is characterized by preserved peristalsis with markedly increased contraction vigor and is defined on high-resolution manometry by a distal contractile integral greater than 8000 mmHg·s·cm in at least 20% of swallows, with exclusion of distal esophageal spasm and achalasia.1–3 In contrast, distal esophageal spasm demonstrates premature contractions with impaired deglutitive inhibition.1,2 In this case, preserved peristalsis and tablet passage (Figures 2-3) argues against classic distal esophageal spasm and favor a hypercontractile physiology. Because radiographic appearances may overlap among esophageal motility disorders, imaging alone is insufficient for definitive diagnosis, and manometric evaluation is required to accurately classify the underlying motor abnormality.3–6 Additional complementary modalities, including timed barium esophagram protocols or functional luminal imaging probe, may be useful when findings are inconclusive.4,5
Management of hypercontractile and spastic esophageal disorders is individualized and symptom-directed. First-line therapy may include smooth muscle relaxants such as calcium channel blockers or nitrates, as well as proton pump inhibitors when reflux overlap is suspected.1–3,6 Refractory cases may require endoscopic or surgical intervention. This case illustrates that a striking “nutcracker” appearance on barium esophagram, while suggestive of an esophageal motility disorder, should not be considered diagnostic in isolation. In the presence of preserved peristalsis and tablet passage, the imaging findings favor a hypercontractile process over classic distal esophageal spasm, but definitive classification requires high-resolution manometry.3–5
Disclosures/Conflicts of Interest
The authors declare that they have no conflicts of interest.
Corresponding Author
David K. A. Donkor, MD
Department of Internal Medicine
Wellstar Spalding Regional Hospital
601 South 8th Street
Griffin, GA 30224, USA
Email: asedakd8@gmail.com