
Background
Blastomycosis is a systemic fungal infection caused by Blastomyces dermatitidis and related dimorphic fungi endemic to regions of North America. Although pulmonary disease is most common, extrapulmonary dissemination occurs in up to 40% of cases, frequently involving the skin and bones. Osseous blastomycosis is uncommon and often mimics traumatic, inflammatory, or malignant processes, leading to diagnostic delays.1
Case Presentation
A 46-year-old woman from the United States Midwest region with a medical history notable for migraines presented initially with left knee pain that developed after a routine gym workout. She denied any significant trauma during the session but reported that the pain had progressively intensified over the next 24 hours, prompting evaluation. An MRI of the left knee demonstrated diffuse marrow edema involving the proximal tibia, thickening of the medial collateral ligament suggestive of a sprain, strain of the popliteus muscle, and a moderate joint effusion. Although these findings were initially interpreted as possibly post-traumatic, the orthopedic consultant raised concern for an occult stress fracture and recommended conservative management, including limited weight-bearing and analgesics.
Over the subsequent days, the patient experienced a notable decline in her overall health. She reported worsening fatigue, diffuse malaise, and shortness of breath on exertion, symptoms she had not previously experienced. During an urgent evaluation in the emergency department, she was found to be hypoxic, and lung auscultation revealed fine crackles localized to the left lower lung field. A CT scan of the chest demonstrated patchy ground-glass opacities without evidence of pulmonary embolism. Because of the respiratory findings and systemic symptoms, she was empirically treated for community-acquired pneumonia.
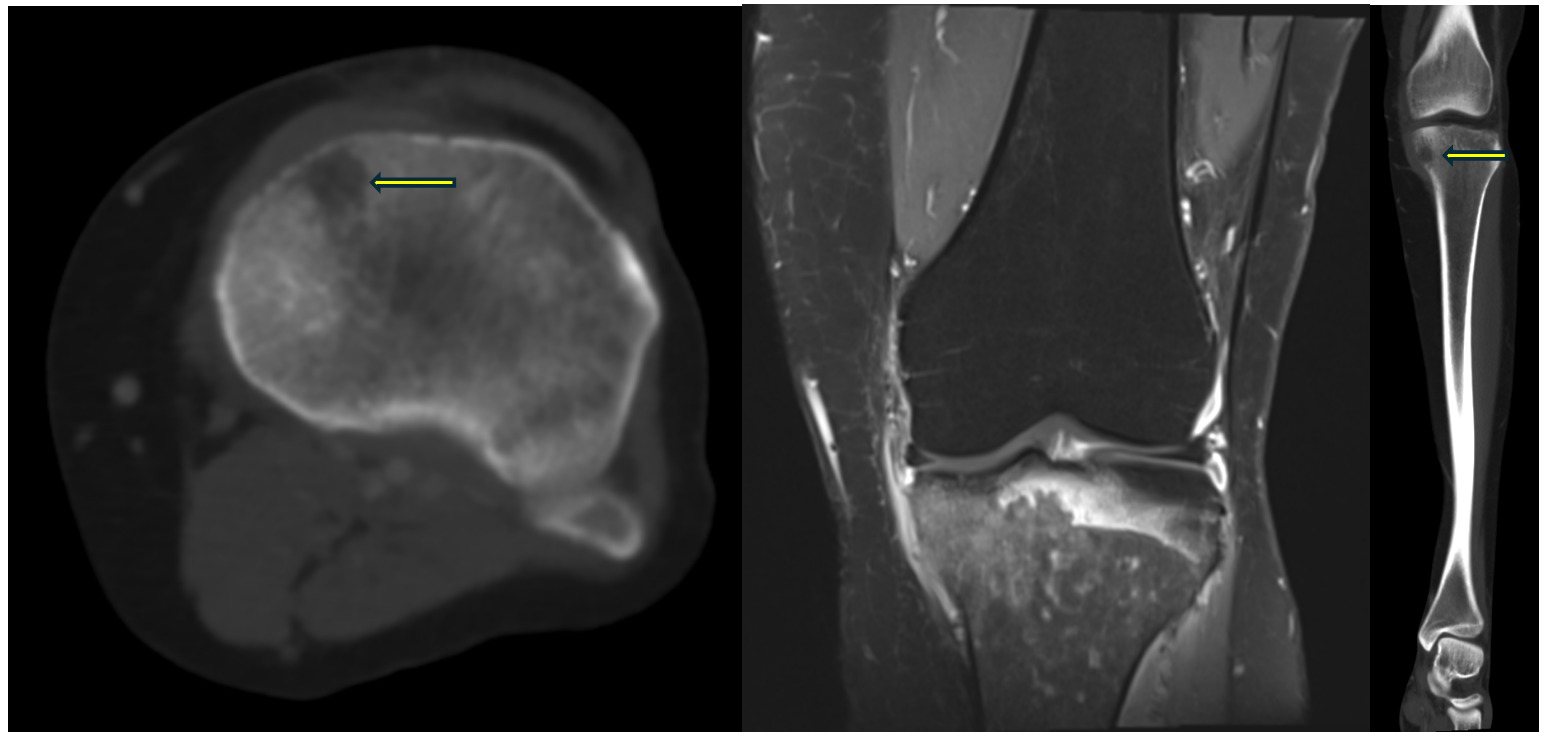
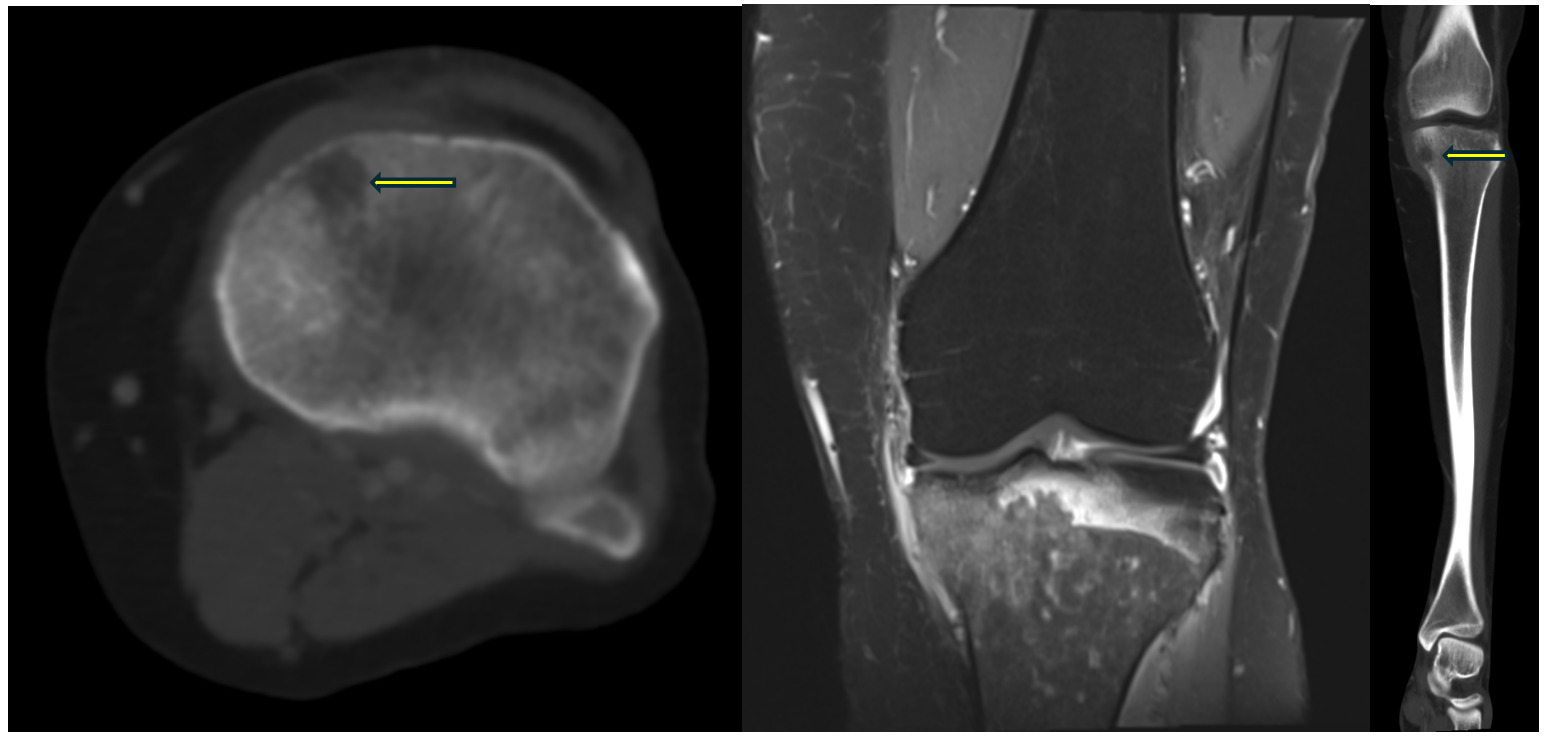
Additional testing, however, revealed an acute occlusive thrombosis of the mid soleal vein on Doppler ultrasonography. She was started on apixaban for venous thromboembolism in addition to the empiric antibiotics. Despite these interventions, her respiratory status and constitutional symptoms continued to worsen. Serial laboratory tests revealed a rising leukocytosis, elevated C-reactive protein, and an increased erythrocyte sedimentation rate, raising concern for a systemic inflammatory or infectious process. A repeat MRI of the tibia demonstrated interval development of a 9-mm lytic lesion with cortical breakthrough and surrounding periostitis (Figure 1). The evolving osseous abnormality prompted hematology consultation due to concern for underlying malignancy, including lymphoma or multiple myeloma. Comprehensive evaluation, including serum and urine immunofixation, did not reveal evidence of monoclonal gammopathy, and a skeletal survey showed no additional lytic lesions.
Given the persistent systemic symptoms, rapid progression, newly identified bone lesion, residing in the United States Midwest, and her reported occupational exposure to building renovation environments, as well as recent travel to the Northern parts of Wisconsin, an infectious disease consultation was obtained. A broad infectious workup was pursued, including testing for Epstein–Barr virus, Histoplasma, Blastomyces, Brucella, Coccidioides, and Mycobacterium tuberculosis. Surprisingly, all results returned negative except for a positive urine antigen for Blastomyces dermatitidis (Supplementary material). Around the same time, the patient developed new cutaneous lesions on her extremities (Figure 2), further supporting the diagnosis of disseminated blastomycosis.

Considering the progressive and rapid multisystem involvement, pulmonary, osseous, and cutaneous, she was promptly started on intravenous amphotericin B for severe disseminated fungal infection. Her clinical course, initially suspicious for mechanical injury and later malignancy, ultimately proved to be a rare presentation of systemic blastomycosis involving the bone. Given her remarkable clinical improvement with intravenous amphotericin B, further testing was not pursued.
Discussion
Blastomycosis is a systemic pyogranulomatous infection caused by Blastomyces dermatitidis and related Blastomyces species, which are thermally dimorphic fungi. These organisms exist as molds in the environment and convert to pathogenic yeasts at human body temperature. They are endemic to specific regions in North America, particularly areas bordering the Great Lakes, along the Mississippi and Ohio River valleys, and portions of the southeastern United States. Inhalation of airborne conidia represents the primary mode of acquisition, after which the fungus transforms into the yeast form within the lungs and may disseminate hematogenously to other organs. Although many infections remain subclinical or mild, approximately 25–40% of symptomatic cases develop extrapulmonary involvement, most commonly affecting the skin, bones, and genitourinary tract.2–4
Among the sites of dissemination, osseous involvement is relatively uncommon yet clinically significant, as it frequently leads to diagnostic delays. Bone blastomycosis ranks as the third most frequent extrapulmonary manifestation, occurring in 14–60% of disseminated cases depending on the cohort studied. The wide range reflects geographic differences in prevalence and variations in diagnostic practices. When present, the disease typically manifests as localized pain, soft-tissue swelling, and occasionally decreased range of motion. Notably, patients may have few or no systemic symptoms, which contributes to misdiagnosis or attribution to traumatic or degenerative musculoskeletal conditions.5–7
The lower extremities, particularly around the knee, including the distal femur, proximal tibia, and fibula, are among the most affected sites. Other frequently involved bones include the vertebrae, ribs, and long bones such as the humerus.6 In a retrospective Canadian series of 45 patients with bone blastomycosis, 73% presented with a solitary osseous lesion, 64% had concurrent pulmonary disease, and 22% reported trauma at or near the affected site. Although trauma does not cause infection, localized injury may attract attention to previously unrecognized fungal invasion or alter local tissue defenses in a way that facilitates fungal proliferation.7
Radiographically, bone blastomycosis may appear deceptively aggressive. Early imaging findings are often nonspecific, sometimes showing only mild osteopenia or subtle periosteal changes.6 As infection progresses, well-defined lytic lesions or more diffuse destructive lucencies develop, frequently accompanied by surrounding soft-tissue inflammation. Cortical breakthrough, periostitis, and adjacent abscess formation are not uncommon. These findings often mimic malignancies, such as lymphoma, metastatic disease, or multiple myeloma, as well as tuberculosis or bacterial osteomyelitis.8 In the spine, vertebral involvement can present with paravertebral abscesses or epidural extension, creating additional diagnostic complexity and potential for neurologic compromise.
Given the broad differential diagnosis and potential for misinterpretation, accurate diagnosis requires integration of clinical, radiologic, and laboratory findings. Identification of the organism may be achieved through culture, histopathology demonstrating broad-based budding yeasts, or non-culture diagnostics such as antigen testing.9 Urine antigen assays are sensitive but may exhibit cross-reactivity with Histoplasma, warranting cautious interpretation.2
Management of blastomycosis depends on disease severity, degree of dissemination, and patient-specific factors such as immune status. The Infectious Diseases Society of America (IDSA) recommends antifungal therapy for all symptomatic infections, regardless of extent. For mild-to-moderate pulmonary or extrapulmonary disease, itraconazole remains the first-line agent due to its efficacy and favorable tolerability profile. More severe disease, characterized by respiratory compromise, extensive osseous involvement, central nervous system spread, or immunosuppression, requires initial treatment with amphotericin B, typically in a lipid formulation to reduce nephrotoxicity.1,2 After clinical improvement, patients transition to oral itraconazole to complete several months of therapy. For individuals unable to tolerate itraconazole or with refractory disease, alternative azoles such, as voriconazole or posaconazole provide effective options.3Ultimately, recognizing bone blastomycosis is crucial, as timely initiation of antifungal therapy significantly improves outcomes and prevents progressive destructive disease.
Conclusion
This case describes a common musculoskeletal complaint that ultimately led to the rare diagnosis of disseminated blastomycosis in an immunocompetent patient, with osteoarticular, pulmonary, and cutaneous involvement. The initial presentation closely resembled a stress fracture or neoplastic process, underscoring the importance of including fungal infections in the differential diagnosis, particularly in endemic regions or in patients with relevant environmental exposures. Early recognition and initiation of appropriate antifungal therapy are essential for optimal outcomes.2,4,8
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest.
Corresponding author
Adrian Umpierrez MD,
Department of Medicine,
Emory University School of Medicine, Atlanta, GA, USA
Email: aumpier@emory.edu