Background
Heart failure (HF) remains a major and growing public health burden, affecting over 6 million adults in the United States, with prevalence projected to increase substantially in the coming decade.1 Heart failure with preserved ejection fraction (HFpEF) now accounts for approximately half of all HF cases, particularly among older adults, and is strongly associated with comorbid conditions such as hypertension, type 2 diabetes mellitus, atrial fibrillation, and obesity. Despite its prevalence, HFpEF has historically posed significant therapeutic challenges due to its heterogeneous pathophysiology and limited response to treatments proven effective in heart failure with reduced ejection fraction (HFrEF). Although this review focuses on HFpEF, Table 1 outlines how the ACC/AHA/HFSA classify heart failure based on ejection fraction.
Recent advances in guideline-directed medical therapy (GDMT) have begun to shift the treatment paradigm for HFpEF, with emerging evidence supporting targeted pharmacologic therapies alongside comprehensive comorbidity management. This review aims to synthesize current evidence on GDMT in HFpEF, focusing on clinically relevant pharmacologic interventions and their application in hospitalized patients. We provide a practical, hospitalist-oriented framework to implement evidence-based therapies and optimize care for this complex and increasingly prevalent patient population.
Pathophysiology of HFpEF
HFpEF is a multifactorial syndrome that differs fundamentally from HFrEF in its underlying pathophysiology. Rather than being driven by cardiomyocyte loss and impaired systolic function, HFpEF develops in the context of systemic comorbidities—such as hypertension, T2DM, coronary artery disease (CAD), chronic kidney disease (CKD), anemia, AF, obesity, and pulmonary disease—that contribute to a chronic low-grade inflammatory state. This inflammation plays a central role in initiating endothelial and microvascular dysfunction, which in turn impairs nitric oxide signaling, reduces capillary density, and promotes myocardial ischemia and stiffening of the ventricle. T2DM has been shown to increase the mortality of HFpEF patients by 30-50%.7,8 This is because T2DM impairs cardiac function by decreasing glucose uptake and uncoupling mitochondrial oxidative phosphorylation, leading to myocardial cell damage and irregular cardiac relaxation patterns. CAD is prevalent in more than 50% of HFpEF patients.8 The risk of cardiovascular death is significantly higher in HFpEF patients with CAD than in HFrEF patients with CAD. This is due to stenosed coronary arteries that reduce coronary flow to the myocardium, leading to decreased diastolic functional reserve. Also, remodeling with compensatory hypertrophy and scarring can occur due to myocardial infarction. AF is a dangerous comorbidity in patients with HFpEF. In fact, if both heart failure and AF coexist, there is an increase in hospitalizations and a two-to-three-fold higher mortality.8 AF is one of the most common predictors of HFpEF development. Also, most people with HFpEF will develop AF at some point. HFpEF and AF are associated with progressive left atrial myopathy.
HFpEF often coexists with CKD, and the two conditions worsen each other’s symptoms—a relationship known as cardiorenal syndrome. CKD causes fluid overload which increases RAAS activity and impairs sodium excretion which worsens congestion. Also, CKD causes inflammation and endothelial dysfunction which promotes remodeling. HFpEF can worsen CKD due to elevated central venous pressure, which leads to congestive nephropathy. Also, the reduced cardiac output from HFpEF impairs renal perfusion, which reduces filtration. As a result, patients with CKD and HFpEF have higher hospitalization rates, worse response to therapies, and higher levels of mortality.9 The main treatment for these patients are SGLT2 inhibitors which can improve HFpEF outcomes and slow down the progression of CKD.9
As endothelial function deteriorates, inflammatory cytokines and oxidative stress stimulate cardiomyocyte hypertrophy and the accumulation of interstitial and perivascular fibrosis. These changes result in increased left ventricular stiffness, which impairs diastolic relaxation and filling. This stiffness is further compounded by abnormal calcium handling and modifications in titin isoforms that shift toward stiffer variants, all of which reduce myocardial compliance.4,10 The elevated filling pressures resulting from these processes lead to pulmonary venous congestion, exertional dyspnea, and fluid overload. Additionally, neurohormonal dysregulation contributes to disease progression. Activation of the renin-angiotensin-aldosterone system (RAAS) and elevated endothelin-1 levels promote vasoconstriction, fluid retention, and increased afterload.5 Although the natriuretic peptide system normally counterbalances these effects through vasodilation and natriuresis, its function is blunted in HF due to enhanced clearance by neprilysin, thereby limiting its protective impact.11 Unlike HFrEF, which is characterized by loss of contractile myocardium with localized replacement fibrosis typically following myocardial infarction, HFpEF features diffuse interstitial and perivascular fibrosis that reflects chronic metabolic and hemodynamic stress rather than direct myocardial injury.12 Ultimately, HFpEF represents a distinct form of heart failure marked by preserved systolic function but impaired diastolic filling, driven by inflammation, vascular dysfunction, and fibrotic remodeling of the myocardium.
Etiologies of secondary HFpEF
Hypertrophic Cardiomyopathy
Two important cardiomyopathic causes of HFpEF are hypertrophic cardiomyopathy and transthyretin amyloid cardiomyopathy. These etiologies are vital to address because they require disease-specific therapies, and early recognition will improve long-term outcomes. Hypertrophic Cardiomyopathies (HCM) are caused by diastolic dysfunction. The ventricle is hypertrophied with reduced compliance, which leads to impaired diastolic relaxation and higher left atrial pressure. This can lead to pulmonary congestion. HCM can present with a LV outflow tract (LVOT) obstruction, which can worsen symptoms.13 Standard therapies for LVOT obstruction have been beta blockers, non-dihydropyridine calcium channel blockers, and sodium channel blockers. However, mavacamten was incorporated into the 2024 ACC/AHA Guideline for the Management of Hypertrophic Cardiomyopathy as a Class I recommendation (Level of Evidence B) for patients with symptomatic obstructive HCM who remain symptomatic despite first-line therapy with beta-blockers or calcium channel blockers.14 Mavacamten works by reducing actin-myosin cross-bridges during contraction, thereby decreasing hypercontractility and LV wall stress.15 Studies showed that mavacamten increased peak VO2 and significantly reduced exercise-induced, resting, and Valsalva-provoked LVOT gradients.16 Traditional therapies such as beta blockers and calcium channel blockers slow heart rate and reduce contractility indirectly. In contrast, mavacamten directly affects the sarcomere by stabilizing myosin heads in a relaxed state, thereby preventing excessive cross-bridging.15 As a result, Mavacamten provides a non-invasive alternative to surgery in the treatment of obstructive HCM. Aficampten is also a cardiac myosin inhibitor that reduces left ventricular outflow tract obstruction and decreases HCM symptoms.17 It was approved in December 2025 for the treatment of symptomatic obstructive HCM. Results from the SEQUOIA-HCM Phase 3 trial demonstrated that aficamten, compared with placebo, significantly improved symptoms and enhanced exercise capacity.17 Although aficamten has demonstrated promising results in the SEQUOIA-HCM trial, it has not yet been incorporated into major society guidelines, and therefore currently lacks a formal class of recommendation or level of evidence designation.17
Transthyretin amyloid cardiomyopathy (ATTR-CM)
Transthyretin amyloid cardiomyopathy (ATTR-CM) is a rare but severe case of restrictive cardiomyopathy caused by transthyretin fibrils in the myocardium.18 Amyloid deposition results in ventricular stiffening and impaired compliance which leads to classic HFpEF symptoms of dyspnea, fatigue, preserved LVEF, and pulmonary hypertension. Patients with ATTR-CM–associated HFpEF have worse outcomes than those with hypertensive HFpEF. Individuals with transthyretin amyloid cardiomyopathy (ATTR-CM) have benefitted from advances in both broadly effective heart failure therapies, including mineralocorticoid receptor antagonists and sodium-glucose cotransporter-2 inhibitors, as well as disease-modifying therapies targeting transthyretin amyloid deposition. Current FDA-approved therapies include the transthyretin stabilizers tafamidis and acoramidis, and the transthyretin silencer vutrisiran.19 Tafamidis became the first FDA-approved therapy for ATTR-CM following the ATTR-ACT trial, which demonstrated reductions in all-cause mortality and cardiovascular hospitalizations.20 Acoramidis was subsequently approved following the ATTRibute-CM trial, which demonstrated favorable effects on cardiovascular hospitalizations.21 Vutrisiran, a small interfering RNA (siRNA) therapy that suppresses hepatic transthyretin production, demonstrated reductions in all-cause mortality and recurrent cardiovascular events in the HELIOS-B trial and received FDA approval for ATTR-CM in 2025.22 Because no head-to-head comparative trials exist, the optimal initial therapy remains uncertain, and treatment selection should be individualized based on cost, access, route of administration, and patient preference regarding route and frequency of administration (oral once per day versus oral twice per day versus subcutaneous injection every 3 months with vitamin A supplementation).19
Obesity and Obstructive Sleep Apnea
Obesity and obstructive sleep apnea (OSA) are key drivers of HFpEF. Obesity is strongly linked because of an increase in hemodynamic load which causes left ventricular remodeling and eventually diastolic dysfunction. Studies have shown that 80% of HFpEF patients are obese and exhibit signs of metabolic syndrome like type 2 diabetes mellitus, hypertension, and dyslipidemia.23 Obstructive sleep apnea (OSA) is also very common in HFpEF patients because it worsens cardiac function by increasing sympathetic tone and leading to chronic hypertension and eventually left ventricular stiffness. Because of the airflow obstruction, there is a drop in intrathoracic pressure which increases afterload and reduces left ventricular filling.24 Current HFpEF management guidelines, including the 2022 ACC/AHA/HFSA heart failure guideline, emphasize treatment of comorbidities such as obesity and obstructive sleep apnea. Weight loss is strongly recommended (Class I) as part of comprehensive risk factor management, while continuous positive airway pressure (CPAP) therapy for OSA is recommended with a Class IIa level of recommendation, based on its ability to improve symptoms and cardiovascular outcomes. GLP-1 agonists have also demonstrated significant benefit. GLP-1 have shown a cardioprotective benefit for HFpEF patients by promoting weight loss, improving insulin sensitivity, decreasing hepatic gluconeogenesis, and diminishing cardiac oxidative stress.23
Diagnostic Algorithms
The HFA-PEFF [Heart Failure Association of ESC diagnostic algorithm, P (pretest assessment), E (Echocardiographic and Natriuretic Peptide score), F1 (Functional testing in Case of Uncertainty, F2 (Final etiology), and H2FPEF [Heavy, Hypertensive, Atrial Fibrillation, Pulmonary Hypertension, Elderly, Filling pressure] are two diagnostic scoring systems that aid in the diagnosis of HFpEF.25 HFA-PEFF is a diagnostic algorithm, while H2FPEF is a probability score.25 One recent study found that H2FPEF is a better diagnostic tool than HFA-PEFF due to its superior accuracy and discriminative ability, particularly when evaluating patients with unexplained dyspnea.25 However, more evidence is needed to establish a clear advantage of one over the other.25,26
Treatment/Management
The management of HFpEF has evolved significantly with the emergence of new pharmacologic therapies; however, translating these advances into meaningful inpatient practice requires a focused, clinically pragmatic approach. While this review highlights the expanding evidence base supporting therapies such as SGLT2 inhibitors, MRAs, ARNIs, and GLP-1 receptor agonists, the applicability of these treatments varies across clinical settings.
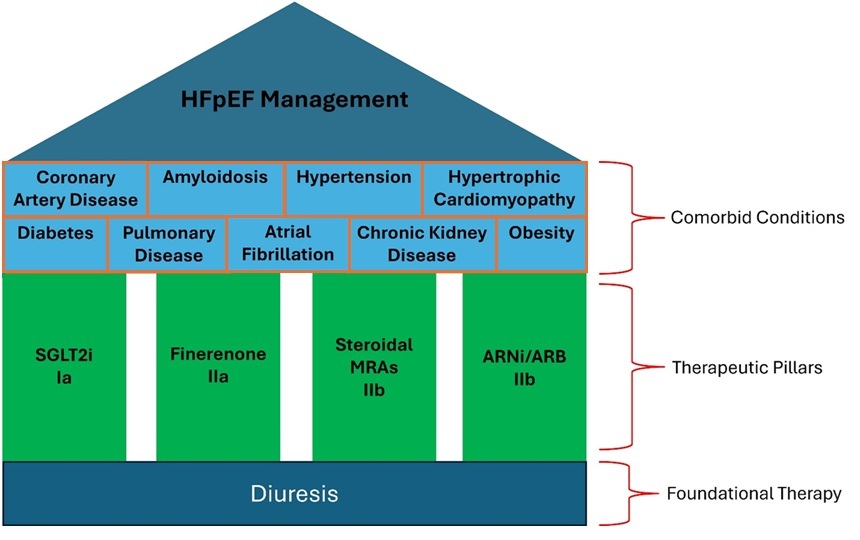
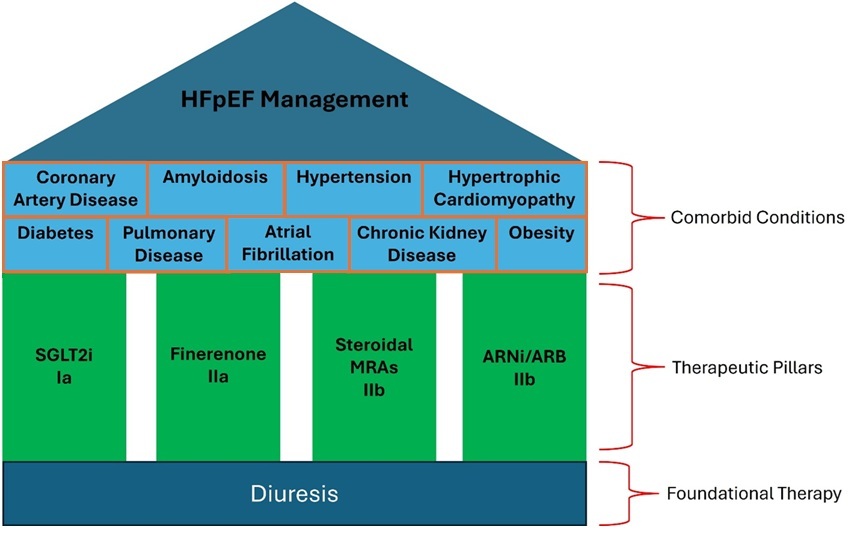
For hospitalists, the primary objective during hospitalization is stabilization of acute decompensation and identification of the underlying drivers of clinical deterioration. Unlike HFrEF, where multiple therapies are routinely initiated during admission, HFpEF management is more heavily centered on volume optimization, blood pressure control, and treatment of comorbidities such as atrial fibrillation, coronary artery disease, chronic kidney disease, and obesity. These comorbid conditions are not only highly prevalent but also frequently represent the primary contributors to hospitalization and disease progression.
Among available therapies, SGLT2 inhibitors represent the most practical and evidence-based option for inpatient initiation, given their favorable safety profile, minimal titration requirements, and consistent reductions in heart failure hospitalizations. In contrast, therapies such as GLP-1 receptor agonists and certain MRAs are more appropriately initiated in the outpatient setting, where longitudinal follow-up and dose titration can be safely achieved. Figure 1 provides a comprehensive management framework for patients with HFpEF.
Guideline-Directed Medical Therapy (GDMT) in HFpEF
HFpEF has historically been challenging to treat due to a lack of clearly effective pharmacologic options; however, several recent trials have informed updates to GDMT. For this review, we evaluated recommendations from the Japanese Circulation Society / Japanese Heart Failure Society (JCS/JHFS 2025), American Heart Association (AHA 2022), and European Society of Cardiology (ESC 2021/2023), as these represent widely cited, contemporary international guidelines that incorporate the most up-to-date clinical trial evidence and offer complementary perspectives across different healthcare systems. Table 2 lists the key randomized controlled trials on pharmacologic management of HFpEF.
Across these guidelines, key management strategies consistently emphasize aggressive control of hypertension and optimization of comorbidities, particularly atrial fibrillation, to improve symptoms and clinical outcomes. Diuretics remain central for symptom relief in patients with volume overload, though close monitoring is required to minimize adverse effects such as electrolyte disturbances and renal dysfunction.16 Notably, the JCS/JHFS recommendations largely align with AHA and ESC guidance, with only minor deviations, as summarized in Table 3.
SGLT2 Inhibitors
The 2025 JCS/JHFS and 2023 ESC guidelines recommend SGLT2 inhibitors for HFpEF with a Class Ia compared with the 2022 ACC/AHA/HFSA guidelines that still assign a Class IIa recommendation.2,16 This stronger endorsement from the JCS/JHFS and ESC reflects accumulating evidence of efficacy and may foreshadow a similar shift in future U.S. guidelines. Supporting this change, a pooled analysis of the EMPEROR-Preserved and DELIVER trials demonstrated that SGLT2 inhibitors, specifically empagliflozin and dapagliflozin, significantly reduced the composite endpoint of cardiovascular death or hospitalization for heart failure.37 Empagliflozin in particular has been associated with a ~30% reduction in HF hospitalizations and consistent benefits across all ejection fraction subgroups.38 Importantly, SGLT2 inhibitors are effective in both ambulatory patients with HFpEF and those with acutely decompensated HF. Meta-analyses further confirm these findings, showing a robust reduction in the composite outcome of HF hospitalization and cardiovascular death (HR 0.80; 95% CI 0.73–0.87).37
ARNI/ARBs
The 2025 JCS/JHFS guidelines mirror the 2022 AHA guidelines by giving ARNIs and ARBs a Class 2b recommendation, particularly for HFpEF patients with LVEF on the lower end of the preserved range.16,39–41 In contrast, the ESC guidelines do not provide specific recommendations for the use of ARNIs or ARBs in HFpEF. Although the primary composite endpoint of total HF hospitalizations and cardiovascular death was numerically lower with sacubitril/valsartan vs valsartan (HR: 0.87; 95% CI: 0.75-1.01), it did not reach statistical significance; however, sacubitril/valsartan is recommended for its comprehensive cardiovascular effects.37 ARBs serve as a viable alternative when ARNIs are contraindicated or not feasible. Careful titration based on patient tolerance, symptoms, blood pressure, potassium levels, and renal function is essential.
Mineralocorticoid Receptor Antagonists
Finerenone, a non-steroidal MRA, carries a Class 1a recommendation in both the JCS/JHFS and ESC guidelines and has been shown to significantly reduce the composite endpoint of cardiovascular death or worsening HF events (including hospitalization and urgent visits) in symptomatic patients with LVEF ≥ 40%.16,27 Steroidal MRAs (e.g., spironolactone and eplerenone) carry a Class 2a recommendation in both the AHA and JCS/JHFS guidelines and may reduce HF hospitalizations in selected subsets of patients with HFpEF, whereas the European Society of Cardiology (ESC) guidelines do not provide specific recommendations for their use in this population.42 While they have not consistently shown improvements in quality of life or exercise tolerance, steroidal MRAs provide balanced diuresis, control of hypertension, and reductions in HF hospitalization rates.16 For all three classes, careful titration based on patient tolerance, symptoms, blood pressure, potassium levels, and renal function is essential.
GLP-1 Receptor Agonists
In patients with HFpEF and comorbid obesity or type 2 diabetes mellitus, semaglutide has been incorporated into the 2025 JCS/JHFS heart failure guidelines with a Class IIa recommendation (Level of Evidence B), reflecting moderate-quality evidence supporting improvement in symptoms and functional status. This recommendation is primarily based on the STEP-HFpEF DM trial, which demonstrated significant improvements in KCCQ scores and weight reduction.16 This change is supported by findings from the 2024 STEP-HFpEF DM trial. The study evaluated adults with HF with LVEF ≥ 45%, type 2 diabetes, and a body mass index (BMI) ≥ 30 kg/m². Treatment with semaglutide 2.4 mg led to significant improvements in heart failure–related symptoms and physical functioning, as measured by KCCQ-CSS, along with meaningful reductions in body weight compared to placebo.43 These results highlight the therapeutic potential of semaglutide in addressing the metabolic and functional impairments common in this HFpEF phenotype.
Beta Blockers
In HFpEF, beta-blockers are not recommended as a primary disease-modifying therapy but are supported by the 2022 ACC/AHA/HFSA guidelines for the management of comorbid conditions such as atrial fibrillation, hypertension, and ischemic heart disease (Class I recommendation for these indications, not HFpEF itself). Their role in ATTR-CM is less clearly defined and requires individualized clinical judgment. Historically, the use of beta-blockers in individuals with ATTR-CM raised concern because of dependence on heart rate to maintain cardiac output, chronotropic incompetence from amyloid infiltration of the conduction system, and autonomic dysfunction. Observational data remain mixed, and beta-blocker discontinuation among studies was high, ranging from 22% to 43%.44 One study reporting no benefit included individuals with more advanced disease and used higher doses of nonselective beta-blockers.44 By contrast, the largest cohort suggested that low-dose beta-blockers (bisoprolol ≤2.5 mg/d) may be beneficial in individuals with an ejection fraction ≤40%. Thus, beta-blockers may be cautiously considered at low doses in those with an ejection fraction ≤40%, especially if needed for rate control of atrial fibrillation, with a low threshold for reduction or discontinuation for intolerance.
Device-Based Therapies
Currently, there are no standard-of-care device-based therapies for HFpEF. However, some therapies, such as interatrial shunt devices and implantable cardioverter-defibrillators (ICDs), may offer benefit in the management of HFpEF. HFpEF causes stiff ventricles, which leads to increased left atrial pressure and eventually pulmonary congestion. Interatrial shunt devices are a promising future treatment because they lower left atrial pressure, especially during exercise.16 The interatrial shunt device allows blood to flow from the left atrium to the right atrium, thereby reducing pulmonary congestion and improving exercise tolerance. Prolonged elevated left atrial pressure is associated with a worse prognosis in HF, so interatrial shunt devices can become an effective therapy.45 Early randomized studies have shown safety and efficacy, and interatrial shunt devices are now in the follow-up phase.15,45
In 1980, Mirowski et al. developed the ICD.26 This important advance has stimulated efforts to identify patients at risk for sudden cardiac death.26 At the highest risk are patients who have had a previous episode of ventricular fibrillation, cardiac arrest, or sustained ventricular tachycardia, and they are candidates for receiving an ICD for secondary prevention. The major risk markers for primary prevention include a family history of sudden cardiac death, left ventricular wall thickness of at least 30 mm, left ventricular apical aneurysm, unexplained syncope, multiple prolonged episodes of nonsustained ventricular tachycardia, extensive late gadolinium enhancement, and left ventricular ejection fraction (LVEF) of less than 50%.26 Patients with overt HCM without high-risk markers should be reexamined at 1- or 2-year intervals for possible emergence of risk markers. The incidence of sudden cardiac death varies inversely with age and is infrequent in patients 60 years of age or older, who may not benefit from placement of an ICD.
Limitations
A key limitation of this review is the heterogeneity of HFpEF as a clinical syndrome, which includes a broad range of phenotypes and comorbidity profiles, limiting direct comparability across trials. Differences in inclusion criteria, ejection fraction thresholds, and endpoints among major randomized controlled trials further complicate cross-study interpretation and may affect generalizability. Although this review includes evidence from RCTs, meta-analyses, and observational studies, variability in study design introduces potential bias in synthesizing outcomes. In addition, guideline recommendations are not fully uniform across major societies, including the AHA, ESC, and JCS/JHFS, reflecting evolving and sometimes differing interpretations of emerging data. Finally, the rapidly expanding HFpEF therapeutic landscape (Table 4) means newer evidence may further refine current conclusions.
Conclusion
Hospitalists play a pivotal role in the management of HFpEF by focusing on acute stabilization, optimizing volume status, and identifying and treating contributing comorbidities. Given the heterogeneity of HFpEF, inpatient care should prioritize addressing factors such as atrial fibrillation, hypertension, renal dysfunction, and ischemia, which commonly precipitate decompensation. While advances in guideline-directed medical therapy have expanded treatment options, not all therapies are immediately applicable in the inpatient setting. SGLT2 inhibitors represent the most evidence-based pharmacologic therapy that can be readily initiated during hospitalization, whereas agents such as GLP-1 receptor agonists are more appropriately incorporated into outpatient management strategies.
A key takeaway from the current evidence is that the impact of inpatient management extends beyond acute stabilization. Hospitalization represents a critical opportunity to optimize medical therapy, address gaps in care, and establish a structured plan for post-discharge management. Without effective transition-of-care strategies, including medication reconciliation, patient education, and timely outpatient follow-up, the benefits of inpatient interventions may be diminished. Ultimately, HFpEF requires a continuum-of-care approach in which inpatient management serves as the foundation for long-term disease control. Hospitalists play a central role in bridging acute and chronic care by initiating appropriate therapies, addressing comorbidities, and ensuring coordination with outpatient providers. Integrating these strategies into routine practice is essential to improving outcomes in this complex and heterogeneous population.
One of the most impactful roles of the hospitalist lies in ensuring a successful transition from inpatient to outpatient care. Early follow-up, medication optimization, patient education, and coordination with primary care and cardiology are essential to improving adherence and reducing readmissions. As the understanding of HFpEF continues to evolve, improving outcomes will depend not only on advancing pharmacologic therapies but also on strengthening continuity of care. A structured, hospitalist-driven approach that integrates inpatient management with outpatient follow-up represents a critical opportunity to enhance long-term outcomes in this increasingly prevalent condition.
Disclosures/Conflicts of Interest
None
Corresponding author
Farzana Hoque, MD, MRCP, FACP, FRCP,
Associate Professor of Medicine,
Saint Louis University School of Medicine, Saint Louis, MO.
Email: farzanahoquemd@gmail.com