Pneumopericardium
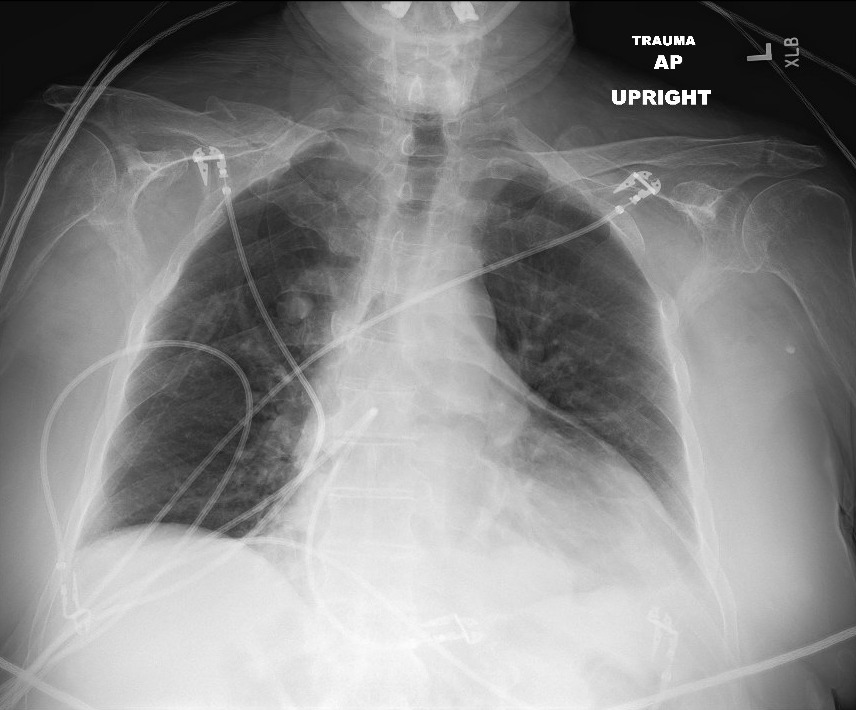
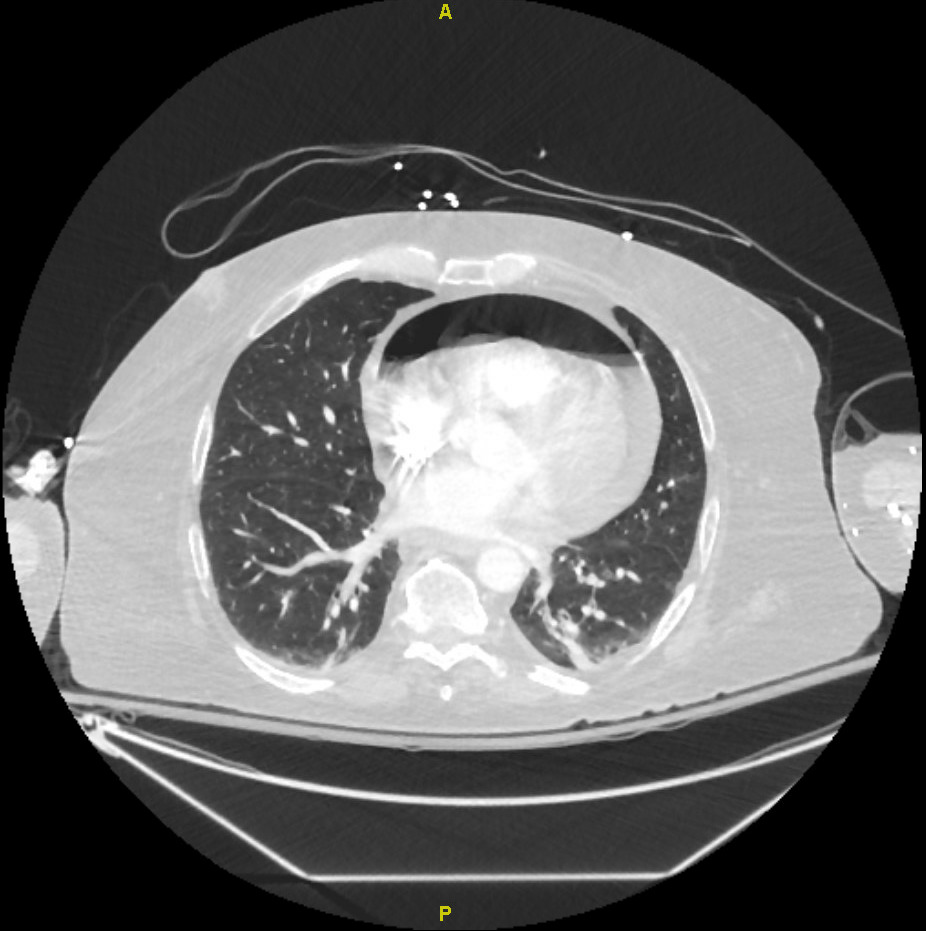
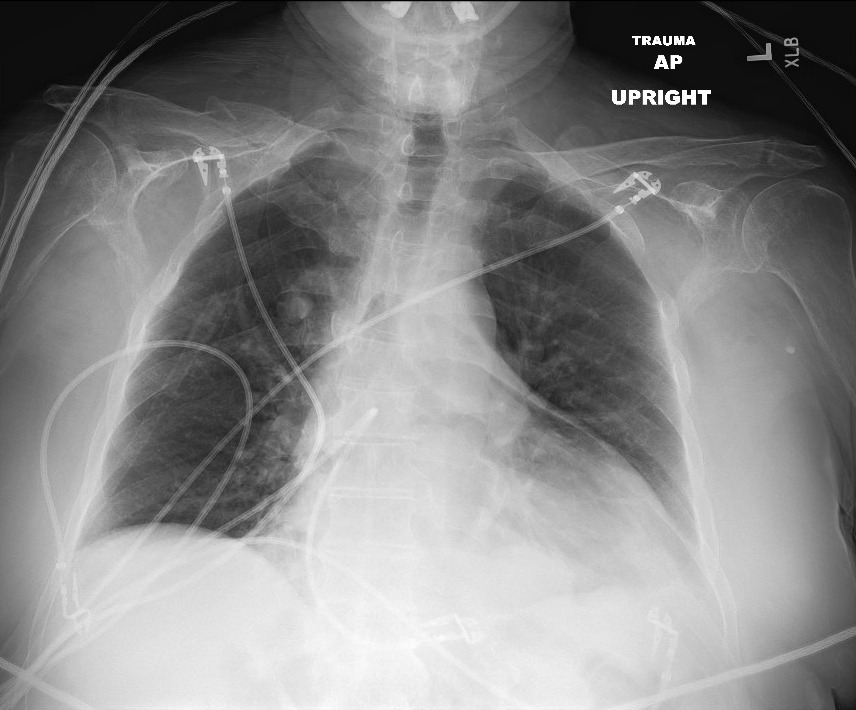
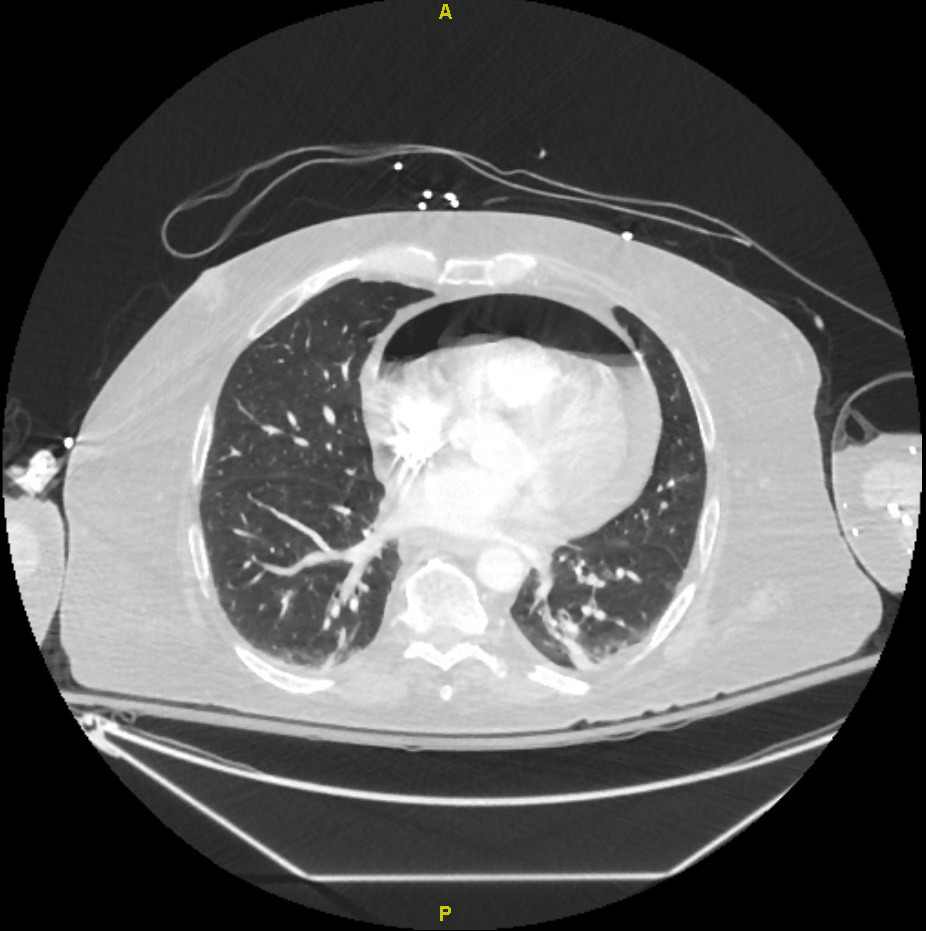
A 62-year-old man with a medical history significant for diabetes mellitus, hypertension, atrial fibrillation, prior pulmonary embolism on apixaban, and obesity status post Roux-en-Y gastric bypass (2014), presented with a 3-day history of progressive shortness of breath and left-sided chest pain. He denied fever, chills, or productive cough. On presentation, he was awake and alert but hemodynamically unstable, with tachycardia (heart rate in the 110s/min) and hypotension (systolic blood pressure in the 70s mmHg). Chest radiography and computed tomography (CT) imaging (Figures 1 and 2) demonstrated findings consistent with pneumopericardium.
An echocardiogram revealed moderate circumferential pericardial effusion along with right ventricular diastolic collapse suggesting tamponade physiology. He subsequently underwent emergent pericardial drainage with pericardial drain placement. Further evaluation revealed a jejunal–pericardial fistula, a rare but recognized late complication of Roux-en-Y gastric bypass surgery. He underwent endoscopic intervention with endovac placement, followed by definitive closure of the fistula after clinical stabilization. Resolution was confirmed with a gastrografin contrast study demonstrating no evidence of leakage.
Pneumopericardium is defined as the presence of air within the pericardial space, which normally contains 15–30 mL of lubricating fluid between the visceral and parietal pericardial layers. Air accumulation in this space typically arises from abnormal communication between the pericardium and adjacent structures, including the pleural cavity, tracheobronchial tree, or gastrointestinal tract. While trauma remains the most common cause, non-traumatic etiologies have been described, including gastrointestinal malignancy, peptic ulcer disease, esophageal diverticula, barotrauma (e.g., mechanical ventilation, vigorous bag-mask ventilation, scuba diving), asthma exacerbations, valsalva maneuvers, infections with gas-forming organisms, thoracic surgery, and complications of prior gastric bypass surgery.1,2 The pathophysiology of pneumopericardium is often explained by the Macklin effect. This mechanism involves an increased pressure gradient between the alveoli and interstitium, leading to alveolar rupture and air dissection along perivascular and peribronchial sheaths toward the mediastinum. If a pericardial defect is present, air may subsequently enter the pericardial sac. Clinical manifestations range from asymptomatic cases to life-threatening complications such as tension pneumopericardium and cardiac tamponade.3
The diagnosis is based on a combination of clinical and radiographic findings. Patients commonly present with chest pain and dyspnea, and may exhibit signs of hemodynamic compromise such as hypotension, as seen in this case. Additional findings can include tachycardia or bradycardia and, in severe cases, cyanosis. When tamponade develops, classic features such as Beck’s triad (hypotension, elevated jugular venous pressure, and muffled heart sounds) may be present. Auscultatory findings may include Hamman’s sign, a precordial crunching sound associated with mediastinal emphysema, or the “bruit de moulin” (mill-wheel murmur), caused by the presence of both air and fluid in the pericardial sac.2
Imaging plays a central role in diagnosis. Chest radiography may demonstrate a radiolucent halo partially or completely surrounding the cardiac silhouette, with sharp delineation of the pericardium by air and, occasionally, the continuous diaphragm sign. CT imaging is the gold standard in equivocal cases, providing detailed characterization and identifying potential underlying causes. Transthoracic echocardiography may reveal characteristic findings such as the “air gap sign,” reflecting cyclical obscuration of cardiac structures during systole, and the “swirling bubbles sign,” indicating an air–fluid interface within the pericardial cavity.4,5
Management depends on the severity and underlying etiology. Mild cases may be managed conservatively with close monitoring and treatment of the precipitating cause. However, in patients with tamponade physiology, urgent pericardial decompression via pericardiocentesis or surgical drainage is required. Placement of a chest tube may be necessary if there is a concomitant pneumothorax. This case highlights a rare but serious cause of pneumopericardium and underscores the importance of prompt recognition and intervention in patients presenting with hemodynamic instability.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding Author
Kwame Dapaah-Afriyie, MD
Professor of Medicine, Clinical Educator
Warren Alpert Medical School at Brown University
Division Director
Division of Hospital Medicine
The Miriam Hospital, 164 Summit Avenue, Providence, RI 02906