The inpatient environment continues to evolve rapidly. Advances in medical science have transformed once-fatal illnesses into chronic conditions, expanded therapeutic options, and prolonged survival across a broad range of diseases. Amid these changes, there has been a growing emphasis on a concept that extends beyond simply living longer: healthspan. As hospitalists increasingly care for older and more medically complex patients, the distinction between lifespan and healthspan is becoming central to clinical decision-making.1–3
Lifespan refers to the total number of years a person lives. It is an objective measure, calculated from birth to death, and is often expressed as life expectancy in population studies. Lifespan does not account for the quality of those years or an individual’s functional status. Healthspan, by contrast, refers to the portion of life spent in good health—free from significant disability, debilitating chronic disease, or major functional limitations. It encompasses physical, psychological, and social well-being and emphasizes an individual’s ability to remain active, independent, and engaged in daily life. While lifespan and healthspan are closely related, they are not synonymous. Healthspan is a more complex and individualized concept, influenced by functional capacity, disease burden, treatment-related complications, and personal perceptions of health and well-being. A patient may live many years with multiple chronic illnesses, yet those additional years may not necessarily be characterized by independence or quality of life.1–3
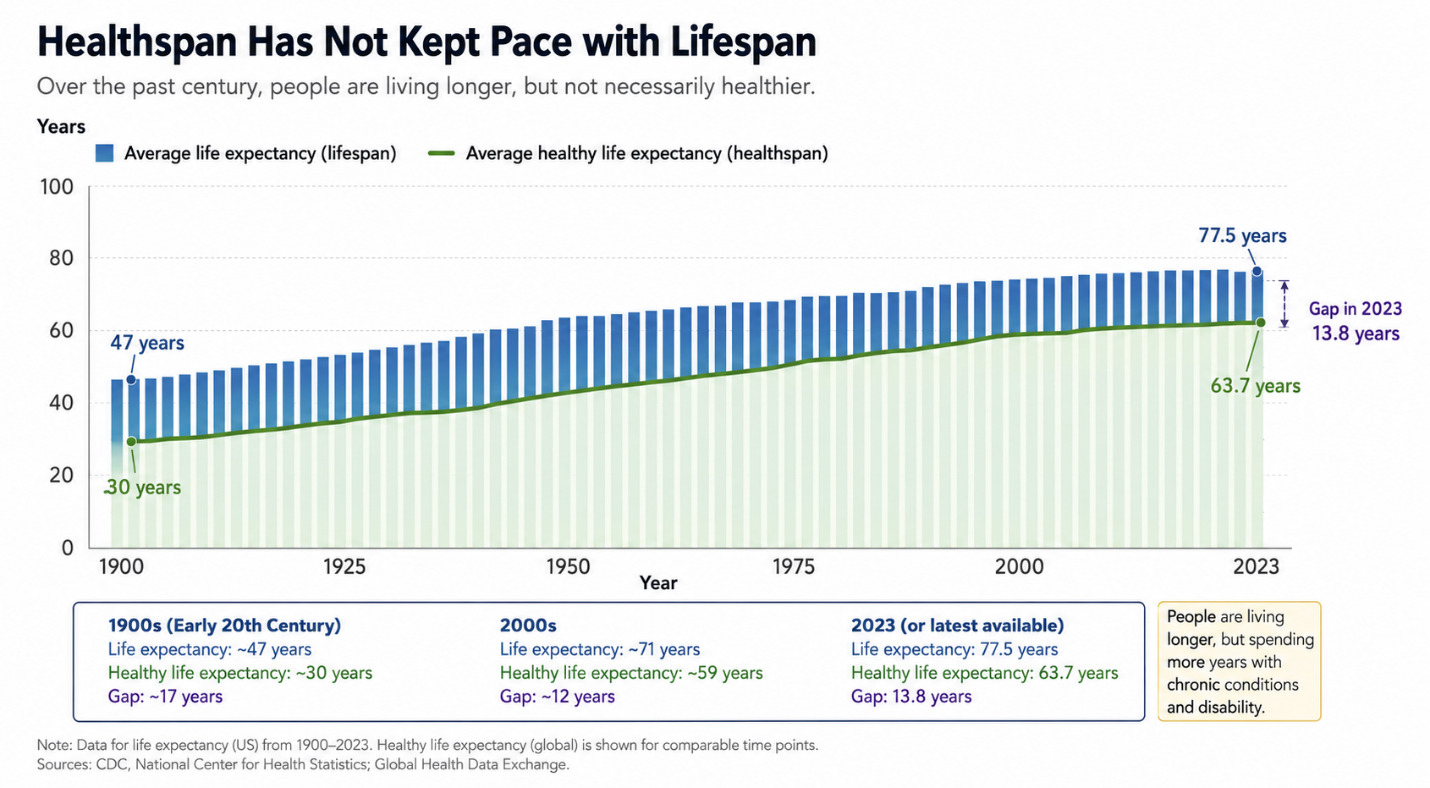
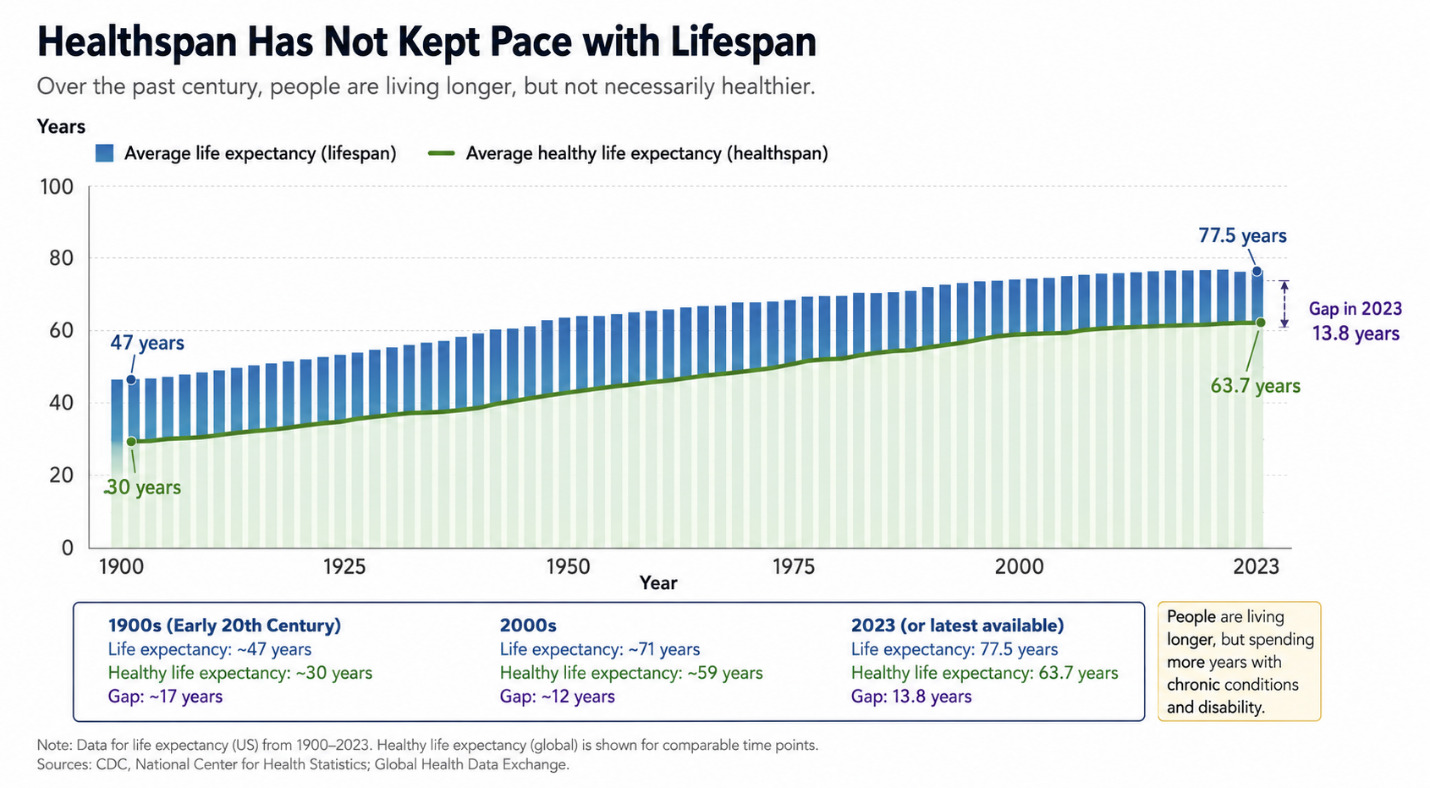
Over the past century, remarkable advances in medicine and public health have substantially increased lifespan. Average life expectancy in the United States has risen from approximately 47 years in the early 1900s to nearly 78 years today. Improvements in sanitation, environmental hygiene, vaccination programs, antibiotics, and preventive medicine account for much of this progress. More recently, advances in cardiovascular medicine, oncology, rheumatology, and immunology have enabled patients to survive conditions that were previously associated with high mortality. However, gains in healthspan have not paralleled gains in lifespan (Figure 1). Many individuals now live for years, and sometimes decades, with chronic diseases such as diabetes mellitus, cardiovascular disease, arthritis, chronic kidney disease, or cognitive impairment. Globally, average life expectancy is approximately 73.4 years, whereas healthy life expectancy is estimated to be only 63.7 years. This discrepancy highlights a growing challenge for modern healthcare: we have become increasingly successful at helping patients live longer, but not necessarily at helping them live better.4
A focus on healthspan shifts the objective of healthcare from simply adding years to life toward adding life to years. Improving healthspan aims to reduce the burden of late-life illness, preserve independence, and enhance overall well-being. Healthspan is influenced by a combination of genetic, environmental, lifestyle, and socioeconomic factors. Consequently, there has been renewed interest in interventions that may delay age-related decline, including dietary modification, physical activity, sleep optimization, and preventive healthcare strategies. At the same time, emerging research in gerotherapeutics is evaluating medications such as metformin, GLP-1 receptor agonists, statins, and SGLT2 inhibitors for their potential to reduce disease burden and improve healthspan.5
The relevance of healthspan is particularly apparent in the inpatient setting, where hospitalists frequently encounter situations that require careful consideration of the trade-offs between longevity and quality of life. Consider the case of an octogenarian with newly diagnosed estrogen receptor-positive, HER2-negative metastatic breast cancer who develops diabetic ketoacidosis after initiation of capivasertib therapy. Although the treatment may offer clinical benefit, the patient ultimately elected to discontinue therapy after considering its long-term implications. Such cases illustrate the delicate balance clinicians must navigate between extending lifespan and preserving healthspan.
The Challenge of Choice
The expanding therapeutic landscape has created an unprecedented number of treatment options for patients with serious illness. Advanced cardiac interventions, biologic therapies, immunosuppressive agents, immune checkpoint inhibitors, and targeted oncologic treatments have demonstrated substantial survival benefits. Yet improvements in lifespan do not always translate into meaningful gains in healthspan. Patients differ considerably in their perceptions of well-being, tolerance of adverse effects, and willingness to accept treatment-related burdens. What constitutes an acceptable trade-off for one patient may be unacceptable for another. Consequently, hospitalists must increasingly engage in nuanced, individualized discussions that align medical recommendations with patient goals and values. Shared decision-making has become essential in helping patients navigate complex choices while preserving autonomy and dignity.6,7
The Challenge of Cognition
The aging population has also led to an increase in the number of hospitalized patients with cognitive impairment. The hospital environment itself often exacerbates underlying cognitive vulnerabilities through acute illness, sleep disruption, medication effects, and delirium. These factors can significantly complicate decision-making. In the absence of clearly documented goals of care or advanced directives, healthcare decisions frequently fall to surrogate decision-makers and powers of attorney. Unfortunately, surrogates may not always have a complete understanding of the patient’s preferences, values, or current functional status. As a result, interventions may be pursued that are inconsistent with the patient’s wishes or unlikely to meaningfully improve either lifespan or healthspan. Tools such as frailty assessments and Eastern Cooperative Oncology Group (ECOG) performance status have become integral to decision-making in geriatrics and oncology. However, these frameworks remain underutilized in many inpatient settings. Greater incorporation of functional status and frailty assessments into routine hospital practice could help clinicians better evaluate prognosis, align treatments with patient goals, and avoid interventions that may prolong suffering without improving quality of life.8,9
The Need for Clinical Collaboration
Addressing healthspan requires a multidisciplinary approach. Primary care physicians, hospitalists, specialists, geriatricians, and palliative care clinicians each have an important role in helping patients make informed decisions that balance longevity, function, and quality of life. Among these disciplines, palliative care occupies a particularly important position. By focusing on symptom management, relief of suffering, communication, and goal-concordant care, palliative care directly contributes to improved healthspan. Despite these benefits, palliative care is often consulted late in the course of illness and is frequently perceived as synonymous with end-of-life care. This limited view diminishes its potential impact and perpetuates misconceptions among both clinicians and patients. Hospitalists should advocate for earlier and more routine integration of palliative care services within inpatient practice. Rather than functioning as an infrequently utilized consultative service, palliative care should be viewed as a core component of the hospital care model. Early involvement can facilitate complex decision-making, improve symptom control, reduce unnecessary interventions, and enhance patient and family experiences.10,11
Looking Forward
As healthcare systems confront an aging population, workforce shortages, rising healthcare utilization, and increasing clinician moral distress, the concept of healthspan offers an important framework for reimagining inpatient care. Hospitalists are uniquely positioned to lead this transition because they are often at the center of conversations involving prognosis, treatment burden, goals of care, and care coordination. The future of hospital medicine should be measured not only by how long our patients live but also by how well they live. Integrating healthspan into clinical decision-making requires a broader focus on function, independence, symptom burden, and patient-defined quality of life.12 It also requires stronger collaboration between hospital medicine and palliative care, greater attention to frailty and cognitive status, and more meaningful conversations about the trade-offs associated with modern medical interventions. In doing so, we remain true to William Osler’s enduring observation: “The good physician treats the disease; the great physician treats the patient who has the disease.” By focusing not only on extending life but also on preserving its quality, hospital medicine can help ensure that the additional years afforded by modern medicine are years worth living.
Corresponding author
Kwame Dapaah-Afriyie, MD
Professor of Medicine, Clinical Educator
Warren Alpert Medical School at Brown University
Division Director, Division of Hospital Medicine
The Miriam Hospital, 164 Summit Avenue, Providence, RI 02906