Introduction
Typhlitis, also referred to as neutrophilic cecitis or neutropenic enterocolitis, was first described in children with neutropenia treated for Acute Myeloid Leukemia.1 Cases have since been reported in adults, primarily in severely immunosuppressed patients undergoing chemotherapy for leukemia, lymphoma,2 and solid tumors, including breast, lung, colorectal and ovarian cancer.3,4 It still has a higher incidence in the pediatric population. Here we describe an immunocompromised patient with lymphoma and common variable immunodeficiency (CVID) who presented with acute abdominal pain and found to have acute typhlitis.
Case Report
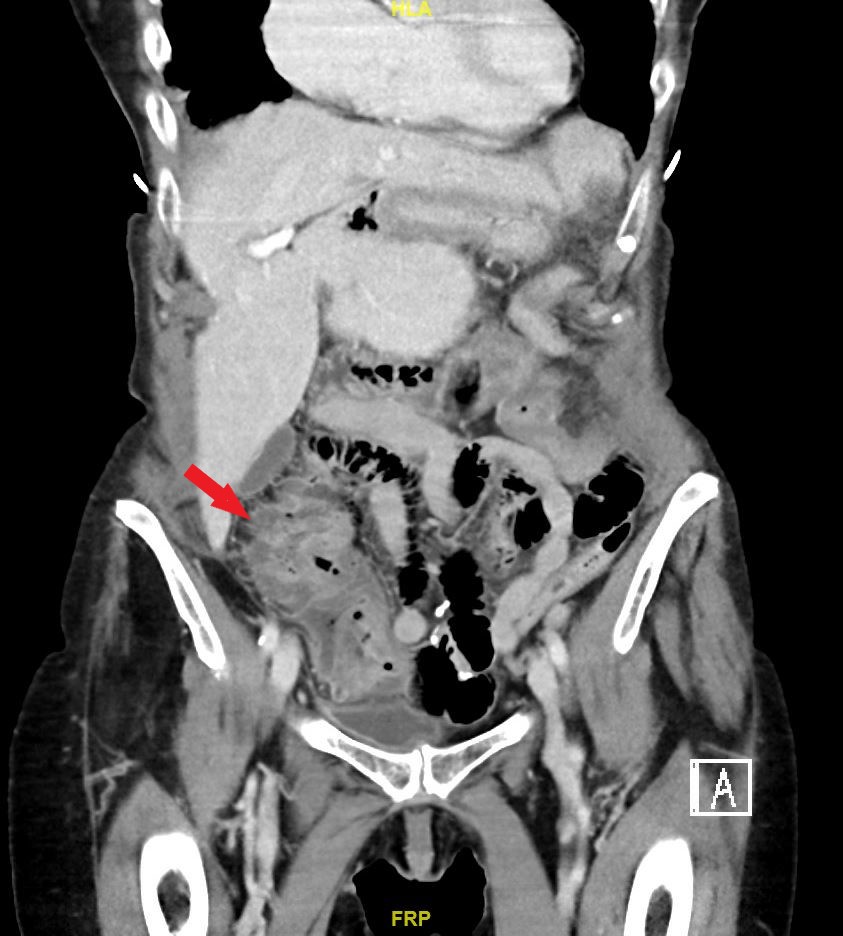
An 82-year-old female with a history of low-grade lymphoma and CVID on intravenous immunoglobulin presented with a 3-day history of fevers, nausea, diarrhea, and right-sided abdominal pain. Her most recent chemotherapy regimen was approximately eight days prior to his presentation. At the time of admission, her temperature was 98.9F, heart rate 65 beats/min, BP 100/56 mmHg, and respiratory rate of 16 breaths/min. Her examination was notable for right lower quadrant abdominal tenderness but no guarding. Her labs were remarkable for hemoglobin of 8.2gm/dl, white cell count 11,000 with an absolute neutrophil count of 490, and platelet count of 89,000. His BMP was remarkable for sodium of 129mEQ/L, Potassium 3.1 mEQ/L, BUN 32mg/dl, and creatinine 1.1mg/dl. CT scan showed diffuse symmetric thickening of the cecum consistent with typhlitis (Figure 1).

She was started on broad-spectrum antibiotics, intravenous fluids with clinical improvement and discharged home on oral amoxicillin-clavulanate.
Discussion
Typhlitis is a severe inflammatory disorder of the intestines that occurs in neutropenic patients. The term typhlitis comes from the Greek word ‘tuphlos,’ meaning cecum or blind gut. Common risk factors are patients with acquired immunodeficiency syndrome, aplastic anemia, myelodysplastic syndromes, multiple myeloma, and cyclic neutropenia. Associated culprit medications include platinum-based chemotherapeutic agents, docetaxel, cytarabine arabinoside, tacrolimus, sulfasalazine, procainamide, and more recently, the monoclonal antibody alemtuzumab.5
Diagnosis is typically made based on a combination of clinical and radiologic findings. To diagnose typhlitis, patients must have fever, abdominal pain, and demonstration of bowel wall thickening by more than 4 mm (transversal scan) or more than 30 mm (longitudinal scan) in any segment by imaging.6 The imaging study of choice is a computed tomography (CT) scan of the abdomen. The typical findings are intestinal dilatation, intestinal wall thickening, and pneumatosis. Some patients with Crohn’s disease may also have mural thickening, mesenteric stranding, and a fat halo sign.7,8 However, the presence of pneumatosis intestinalis in typhlitis is the distinguishing feature between both conditions.
Typhlitis has a reported mortality rate of 40-50%.6 Its early diagnosis and management are therefore crucial. The pathogenesis is believed to be due to a combination of ischemia, infection, and associated mucosal hemorrhage. Neutropenia associated mucosal disruption resulting in inflammation, bacterial translocation resulting in worsening inflammation, edema, and wall thickening. Most conditions tend to be polymicrobial. However, the most common organisms isolated include Pseudomonas aeruginosa, Escherichia coli, Klebsiella spp., Clostridium spp., and enterococci.9 The predilection for the cecum is due to the relative lack of vascularization, although cases involving other colonic sites have been described.
The management is mainly conservative and involves intravenous hydration, broad-spectrum antibiotics, bowel rest, and supplemental nutrition. Electrolytes should be maintained within normal limits, culprit medications discontinued, and GC-CSF is needed in some cases to enhance recovery from neutropenia. Indications for surgery include sepsis needing source control, abscess formation or perforation, and persistent GI bleed. Pitfalls to avoid include not attributing this condition solely to Clostridium difficile colitis in patients whose stools may be colonized with Clostridium difficile (positive PCR results), distinguishing this from Crohn’s disease exacerbation, and being mindful of cases without significantly associated neutropenia due to concurrent use of prednisone.10
To our knowledge, this is the first reported case of typhlitis in a patient with CVID. The increasing use of immunosuppressants in managing inflammatory bowel diseases, multiple sclerosis, and other autoimmune disorders may result in detecting more cases of typhlitis in the non-oncological patient population. A high index of clinical suspicion and increasing awareness among physicians are required to ensure timely diagnosis and prompt management. In the absence of timely diagnosis and management, patients may develop septic shock or perforation of the cecum. An interprofessional approach may be necessary to prevent complications and improve outcomes.
Corresponding author:
Kwame Dapaah-Afriyie
Professor of Medicine, Clinician Educator
Warren Alpert School of Medicine at Brown University
Division of Hospital Medicine
The Miriam Hospital, 164 Summit Avenue, Providence, RI 02906
Tel: 401-793-2104
Fax: 401-793-4047
Email: kdapaahafriyie@lifespan.org