



INTRODUCTION
Timely discharge of medically-ready patients from acute care hospitalization can reduce the strain on hospital resources and limit patient exposure to iatrogenic harm.1 While only two percent of adult hospitalizations in the most recent National Inpatient Sample (2001–2012) were prolonged, defined as 21 days or longer, these patients accounted for over 14% of hospital days and are attributed to over $20 billion in healthcare spending annually.2 A study examining long-term hospitalizations found that from 2001 to 2012, the average acute length of stay (LOS) for long-term hospitalizations in the United States decreased slightly from 27 days to 26.8 days while the cost per hospitalization increased significantly.2 One challenge in timely discharge from acute care is that the dearth of uniform guidelines and standardization during discharge leaves most decisions to be made on a case-by-case basis.3
Timely discharge has become more critical during the COVID-19 pandemic as it increases the availability of acute care beds, decreasing hospital burden and reducing the potential for hospital-based viral transmission.4 A smooth transition is also important since hospitalized COVID-19 patients may need post-acute care to support their recovery. For example, COVID-19 patients treated in the Intensive Care Unit (ICU) and receiving supportive ventilation are at risk of developing Post-Intensive Care Syndrome and may suffer long-term health consequences after discharge.5 Some hospitalized COVID-19 patients may require readmission after discharge, with the Centers for Disease Control reporting a 9% same-hospital readmission rate.6 This rate is higher in patients who were discharged to post-acute care facilities compared to home or self-care. New regulations and the strain on capacity have prompted post-acute care facilities to make adaptations, such as transforming rooms into isolation and quarantine spaces.4
There have been limited studies examining the effect of the pandemic on patient transitions to post-acute care.4 Given the overwhelming nature of COVID-19 and the sharp rise in demand for acute care beds, it is essential to identify and analyze barriers to discharge. Thus, the objective of this study was to analyze barriers to discharge for a subset of patients identified on multi-disciplinary rounds at an urban medical center (1,162 total beds) as having a barrier to discharge before or during the pandemic. A tracking tool was developed by the Care Coordination/Clinical Resource Management department to track these patients and inform post-acute care transitions. We analyzed the relationship between LOS and factors affecting discharge, including identified barriers, discharge disposition, and patient age, for the two periods (before and during COVID-19) to elucidate the impact of the pandemic on timely discharge.
METHODS
The Care Coordination/Clinical Resource Management department (“Care Coordination”) at the Johns Hopkins Hospital created a standardized list of 14 categories of barriers to discharge in late 2019 to track difficulties discharging adult patients from its medicine, surgery, and neurology units (Table 1a). This initiative aimed to identify barriers to discharge and improve transitions to post-acute care, including skilled nursing facilities (SNFs), rehabilitation facilities, home healthcare, home/self-care, and transfer to other hospital facilities (Table 1b). Care Coordination’s Case Managers and Social Workers identified patients with at least one barrier to discharge during daily multi-disciplinary rounds and reviewed cases at a weekly meeting to develop strategies to overcome these barriers. Throughout this process, data was manually collected, including the identified barriers to discharge, disposition, and patient characteristics (i.e., age, primary payer, department). Up to three barriers per patient were recorded. The “COVID-19” barrier was a new barrier identified during the pandemic that encompassed a number of situations complicating discharge, including suspected positive, awaiting testing, and policies that closed post-acute facilities to admission. Post-discharge, the total LOS was logged in the dataset as a standardized measure of hospital stay duration.
This study analyzed the barriers to discharge data collected by Care Coordination in a six-week baseline period before COVID-19 became pervasive in US hospital populations (February 1–March 15, 2020) and in a six-week period when the prevalence of COVID-19 had risen in hospitals (April 1–May 15, 2020). Patients in this dataset were or were soon to be medically ready for discharge and experienced barriers to discharge. The institutional IRB determined that this quality improvement project did not constitute human subjects research and was exempt. Patients in this dataset who were in the hospital during both periods were classified based on their admission date. This analysis included 64 patients in the baseline time period and 68 patients in the COVID-19 period. LOS information was updated as of August 2020, and patients who remained hospitalized at that time were recorded as having the LOS at the end of the study period.
This study investigated the relationship between LOS and factors affecting discharge for two periods (before and during COVID-19). Outliers in each period were identified and excluded from the analysis. Qualitative analyses were used to describe the distribution of conditions affecting discharge for each period, including type and number of barriers to discharge and discharge disposition. Total LOS was used as the outcome variable, and all analyses were run using Stata 17. We used a multivariable linear regression model to analyze the association between LOS and independent predictor variables including age, the number and type of discharge barriers, discharge dispositions, and time period (before vs. during COVID-19).
RESULTS
Discharge Barriers
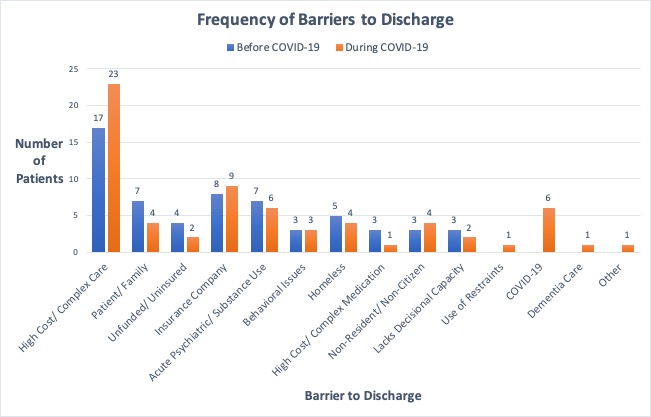
In the baseline period, the most common barrier to discharge was “High Cost/Complex Care Needs” (17 patients; 28%), followed by “Insurance Company” (8 patients; 13%) (Figure 1). The third most common barrier to discharge was tied between “Patient/ Family” and “Acute Psychiatric/Substance Use/Alcohol Use” (7 patients; 12%). The barriers to discharge with the longest average LOS were “Lacks Decisional Capacity” (50 days) and “Non-Resident/ Non-Citizen” (46 days). In the COVID-19 time period, the most common barriers to discharge were “High Cost/Complex Care Needs” (23 patients; 34%) and “Insurance Company” (9 patients; 13%). The third most common barrier to discharge was tied between “COVID-19” and “Acute Psychiatric/Substance Use/Alcohol Use” (6 patients; 9.0%) (Figure 1). The barriers to discharge with the longest average LOS were “Dementia Care Needs” (90 days) and “Use of Restraints” (64 days) (Figure 2).
_vs._during_covid.jpg)
_vs._d.jpg)
While the most common barriers to discharge in both time periods remained “High Cost/Complex Care Needs” (28% before vs 34% during COVID-19) and “Insurance Company” (13% for both periods), there were differences in other barriers to discharge between the two time periods. Barriers to discharge that were common during the baseline time period, such as “Patient/Family” became less common during the COVID-19 time period (12% vs 6.0%) while “COVID-19” became the third most common barrier (9.0%).
Discharge dispositions
In the baseline time period, the most common dispositions among patients captured in this dataset were “Skilled Nursing Facility” (19 patients; 32%), “Self-Care” (11 patients; 18%), and “Home Health Services” (9 patients; 15%). In the COVID-19 period, the most common dispositions were “Skilled Nursing Facility” (24 patients; 36%), “Self-Care” (16 patients; 24%), and “Home Health Services” (11 patients; 16%) (Figure 3)
_vs._during_covi.jpg)
The dispositions with the longest average LOS in the baseline period included “Chronic Hospital/Unit” (83 days), “Rehab” (66 days) and “Expired” (61 days) whereas the discharge dispositions during the COVID-19 period with the longest average LOS were “Rehab” (39 days), “Home Health Services” (33 days), and “Skilled Nursing Facility” (27 days) (Figure 4). The six patients with “COVID-19” as a barrier to discharge had dispositions of “Skilled Nursing Facility” (2 patients), “Rehab” (2 patients), “Self-Care” (1 patient), and “Home Health Services” (1 patient).
_vs._.jpg)
In this study, the three most common discharge dispositions were not affected by the start of the COVID-19 pandemic. In both periods, the most common discharge dispositions were “Skilled Nursing Facility” (32% before vs 36% during), “Self-Care” (18% before vs 24% during), and “Home Health Services” (15% before vs 16% during).
Length of Stay
A multivariable linear regression model that controlled for age and discharge barriers found that patients who had three identified barriers experienced a significant increase in average LOS from the period before COVID-19 (43.5 days) to the period during COVID-19 (70.3 days) (p<0.001). In contrast to this finding, the average LOS for all patients in this dataset decreased from 35.0 days during the baseline six-week period before COVID-19 to 28.1 days during the six-week period during COVID-19. However, this result was not statistically significant (p=0.24) (Figure 5).
_vs._during_covid-19_(apr_1--may_15_.jpg)
DISCUSSION
This study found that acute care patients with three identified discharge barriers experienced a significant increase in average LOS during the COVID-19 period compared to before COVID-19. In contrast, the average LOS for all acute patients with identified barriers in this dataset decreased in the period during COVID-19 compared to before the pandemic. The differences in average LOS between the two periods may have been affected by initiatives to increase acute care capacity during COVID-19, including elective surgery postponement, admission policy changes at post-acute care facilities, and alternative placement arrangements to grow inpatient capacity.
At the start of COVID-19, SNFs had strict and evolving requirements for accepting patients in order to keep existing patients and staff safe and comply with federal and state guidelines.7 Stricter regulations for transfer between hospital units also reduced internal transfers during the pandemic. Meanwhile, the Department of Health and Human Services issued emergency waivers that modified or suspended select federal requirements in order to facilitate timely discharge. One Centers for Medicare and Medicaid Services (CMS) waiver waived certain requirements related to hospital discharge planning for post-acute care services.8 In addition, the CMS guideline requiring a three-day hospitalization prior to SNF admission was waived.9 PPE shortages and limited COVID-19 testing capacity in post-acute care facilities early in the pandemic could have affected LOS and the number of patients discharged to post-acute care.10
These policy changes in acute care discharge could explain the greater number of patients who had a LOS ≤10 days in the period during COVID-19 (16 patients; 24%) compared to the period before COVID-19 (7 patients; 12%). In contrast with this trend, the increase in average LOS for patients with three barriers may suggest that the complexity of these patients and the interaction of multiple barriers may have limited the ability to accelerate discharge plans during the pandemic despite the need for greater availability of acute care beds.
There were also significant changes in Emergency Department (ED) visits and admission rates during COVID-19 because of changing hospital policies and patient behavior. A study of 24 EDs in five states found a decrease in annual ED visits ranging from 41.5% to 63.5%, and hospital admission rates correlated with state-level COVID-19 case rates.11 Similarly, the Kaiser Family Foundation reported that 48% of Americans delayed care themselves or had a family member delay medical care during the pandemic. Of those delaying medical care, 11% reported worsening of their medical condition due to delayed care.12
Since our study was conducted early in the pandemic, delay in seeking care due to COVID-19 could have filtered out long-stay patients from the study population, so an increase in LOS was only observed for complex patients with multiple identified barriers. It has been shown that delay in medical care could lead to increased severity of illness in hospitalized individuals as well as increased morbidity from non-COVID-19-related illnesses.13 Acute care data from China at the start of COVID-19 showed that reduced admissions for strokes were paired with higher NIHSS scores upon hospital arrival, increased severity, and delays in acute ischemic stroke care after hospital arrival.14 This suggests that the average LOS may increase for all acute patients later in the pandemic due to delayed presentation at more advanced stages of the disease.
Limitations of this study include that this analysis was conducted on a specific subset of patients with barriers to discharge identified by Care Coordination case managers and social workers. Therefore, analysis findings are restricted to patients in this dataset and not inclusive of all acute care patients at an urban medical center before and during COVID-19. There are also limitations in tracking and measuring the outcome variable of ‘duration of delayed discharge’. LOS was used as the outcome variable affected by challenges in discharging patients, but it is not equivalent to a measurement of delayed discharge. This limits the interpretation of the results, as it is not evident if the barriers to discharge that require intervention are those most frequently recorded or those associated with longer LOS. The use of a delayed discharge outcome measure would help inform future intervention.
In conclusion, this study examined data from two time periods, before and during COVID-19. The participants for the study were a subset of adult patients in the medicine, surgery, and neurology units experiencing barriers to discharge at the time they were or were soon to be medically ready for discharge. Patients with three barriers experienced an increase in average LOS during the COVID-19 period, while the average LOS of all patients in this dataset decreased during the pandemic. These differences in LOS may have been influenced by changes in care patterns and regulatory factors that aimed to address identified barriers to discharge and increase the availability of acute care beds. These study findings could inform discharge planning for patients facing specific barriers to discharge and guide the next steps in quality improvement. For example, the Care Coordination discharge tracking tool utilized in this study has now been integrated into the institutional electronic health record, EPIC and similar tools have been utilized elsewhere.15–18 This tool makes it possible to track inpatients with barriers to discharge and analyze common discharge barriers at individual hospitals and system-wide. Other steps that could decrease LOS for patients include strengthening relationships with post-acute care facilities and using a system-generated report to review long-stay cases with potential discharge barriers. Further assessment of the interaction of multiple barriers for complex acute patients and the impact of the COVID-19 pandemic on hospital stay could inform additional strategies for timely discharge.
DISCLOSURES/ CONFLICT OF INTEREST
The authors declare they have no conflicts of interest.
FUNDING
This research did not receive any funding from agencies in the public, commercial, or not-for-profit sectors.
Corresponding Author
Grace Xiao
733 N. Broadway #147
Baltimore, MD 21205
gracexiao@jhmi.edu