Background
Cardiovascular disease remains a leading cause of death in the United States and imposes significant costs on our health care system.1–3 Coronary artery disease is the primary driver of overall cardiovascular disease burden. Fortunately, mortality has improved in patients presenting to the hospital with acute myocardial infarction (AMI).4 The adoption of cardiac biomarkers has facilitated more rapid recognition of AMI, allowing clinicians to better triage patients and enact evidence-based management strategies. Initial serum troponin assays were not sensitive enough to exclude an AMI within the first few hours of presentation, which led to the development of high sensitivity assays, now widely used in clinical practice.5
With implementation of high sensitivity assays, hospitalized patients are frequently observed to have an elevated troponin value.6 As a result, major cardiovascular societies have had to continually update the definition of myocardial infarction, with the most recent iteration released in 2018. A key component of the 4th Universal Definition of Myocardial Infarction is the distinction between myocardial infarction and myocardial injury, the former requiring the presence of an elevated troponin value and the presence of ischemia (indicated by clinical, electrocardiographic and echocardiographic correlates), and the latter defined as detection of a cardiac troponin value above the 99th percentile upper reference limit in the absence of ischemic signs.7 Myocardial injury is an increasingly recognized clinical entity, and, when combined with type 2 myocardial infarction (MI), comprises the majority of elevated troponin values seen in an emergency department.8 A type 2 MI is caused by myocardial oxygen supply-demand mismatch with resulting ischemia. Interestingly, patients who suffer a type 2 MI or myocardial injury event have higher short-and long-term mortality rates and have similar rates of cardiovascular death as compared to patients admitted with a type 1 MI.8–10
With increasingly sensitive troponin assays and changing troponin-related nomenclature, we have observed a wide variety of terms used in clinical practice to describe elevated troponin levels. Imprecise use of descriptive language may create confusion about the etiology of an elevated troponin level and may contribute to uncertainty regarding appropriate management. Therefore, the aim of our study was to characterize the range of terms used to denote an elevation in troponin levels, and to assess the frequency with which each term was used in hospital discharge summaries. We also sought to identify instances of potentially conflicting terminology.
Methods
Study Population and Setting
In this retrospective chart review, we included all patients admitted to three hospitals within the largest healthcare system in Rhode Island – an academic tertiary care hospital, an academic community hospital, and a smaller private community hospital – in 2018. Inclusion criteria included age ≥ 55 and ≤ 65 years old and admission to and discharge from the medical floor only (i.e., patients did not require a step-down or intensive care unit). We excluded patients managed on cardiology or non-medical services. Patients in the sample had to have at least two cardiac troponin I (cTnI) measurements, with at least one value measuring above the 99th percentile of the upper reference limit. The troponin also had to demonstrate a rise-and-fall pattern to exclude patients with chronically elevated troponin levels, as in chronic kidney disease for example. For patients with more than one hospitalization during the study period, only the last encounter was included.
Data Extraction
We reviewed text from three sections in the discharge summary: the problem list, the hospital course, and for patients admitted to a teaching service, the attending attestation. The attending attestation, when present, was combined with the hospital course for analysis. Two authors (KC and RG) identified any terms that referred to an elevated troponin level. We did not include terms that reported only a numeric troponin value (e.g., “troponin was 1.2”). Terms with minor variations in language or spelling were considered to be the same term (e.g., “elevated troponin” and “troponin elevation;” “Non-ST-elevation myocardial infarction (NSTEMI) type 2” and “type 2 NSTEMI;” “troponinemia” and “troponemia”). We did not adjudicate the troponin terms to determine if they accurately reflected clinical events during the hospitalization. The authors double-coded 10% of the sample to assess inter-rater reliability (kappa = 0.92).
Statistical Analysis
We used descriptive statistics to calculate counts and percentages. We grouped troponin terms by whether they 1) included a description without reference to abnormality; 2) referred solely to an elevation without mentioning injury, ischemia, or infarction; 3) referred to ischemia or demand without mentioning infarction; or 4) referred to infarction or acute coronary syndrome. The study was approved by the health system institutional review board.
Results
A total of 257 patients were included in the sample. Approximately two-thirds of discharge summaries (169/257, 65.7%) included a troponin term. We identified 19 distinct troponin terms (Table 1). Three of the 19 terms used descriptors that implied a normal troponin level (e.g., “flat troponin”). Seven terms described an abnormal elevation without specifically referencing myocardial injury, ischemia, or infarction as the etiology (e.g., “troponin bump”). The remaining terms referenced ischemia or infarction (e.g., “NSTEMI”).
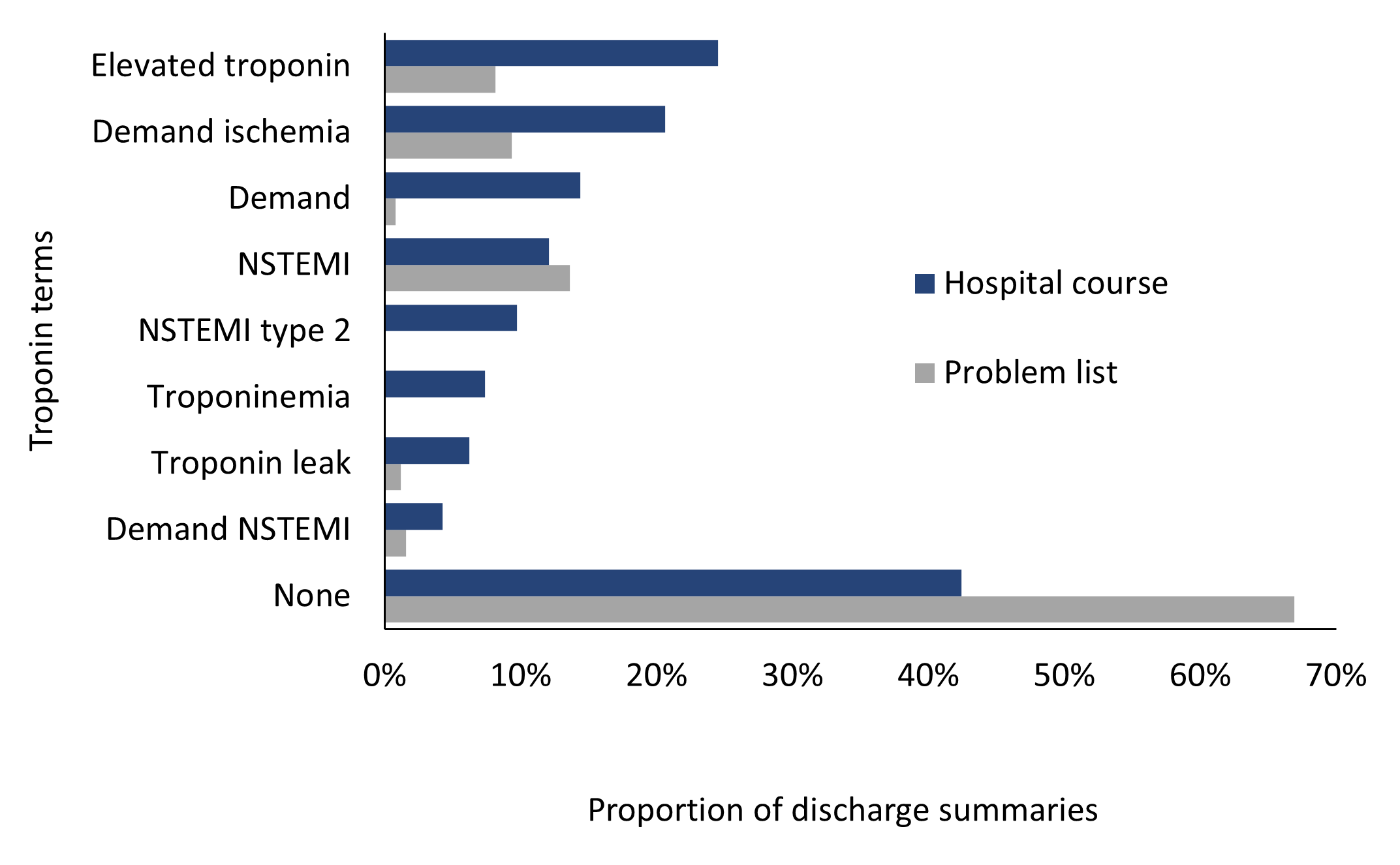
Comparing the hospital course to the problem list, 58% of charts (148/257) had troponin terms in the hospital course while 33% (85/257) of problem lists had troponin terms (Figure 1). Among all discharge summaries with a troponin term, the term used in the highest proportion of hospital course narratives was “elevated troponin,” followed by “demand ischemia” and “demand.” “NSTEMI” was identified in the highest proportion of problem lists, followed by “demand ischemia” (Figure 1).

Discussion
We found that hospital clinicians used a wide variety of terms to describe an elevated troponin level in their discharge summaries and that a third of discharge summaries did not include any reference to a troponin elevation. A substantial proportion of the troponin terms we identified included qualifying language that is potentially minimizing, such as “troponin bump” or “troponin leak.” In other instances, the elevated troponin description was accompanied by language such as “stable,” “minimal,” or even “negative,” despite being elevated beyond the upper limit of normal. A troponin value above the 99th percentile is associated with adverse short- and long-term outcomes regardless of etiology.8–10 It may serve as an important data point for clinicians caring for the patient during the hospital stay and after discharge. Hospital management and post-hospitalization follow up of patients with myocardial injury or type 2 MI is frequently varied.11 Standardizing troponin terminology may prompt further outpatient investigation into cardiac risk factors and risk reduction strategies.
We also found instances of clinicians using a specific troponin term and then providing evidence to the contrary within the same discharge summary. For example, in one hospital course narrative, a clinician gave a diagnosis of “NSTEMI” and also described the absence of clinical correlates required to diagnose ischemia. In another case, a patient was said to have suffered an “NSTEMI” in one part of the hospital course, and the troponin elevation was attributed to chest trauma elsewhere in the hospital course. Conflicting language in the discharge summary may make post-discharge management of these patients more challenging for outpatient clinicians.
Importantly, just over one-third of the records had no troponin terms in the discharge summary, despite those patients having at least one abnormal troponin level during their hospitalization. There are several possible explanations for this observation. 21st century clinical care is inherently complex,12 and admitted patients are often treated for several medical problems, which may deter clinicians from mentioning an elevated troponin level in discharge documentation. This omission might be related to a desire to keep discharge summaries succinct, with the elevated troponin interpreted as a manifestation of the severity of the patient’s sepsis diagnosis, for example, instead of as a separate issue during the hospital stay. Or it may be due to an underappreciation of the prognostic importance of an elevated troponin level. Loss of key information during clinician changes in a patient’s hospitalization may also contribute.
We note several important limitations to our study. The study period was prior to publication of the 4th Universal Definition of MI,7 and thus we cannot assess whether this latest guidance has changed practice. Clinical documentation queries may affect the use of certain troponin-related terms in the chart; therefore, we recommend clinicians who are up-to-date on recent consensus in the field guide implementation of troponin-related documentation queries. Our study population specifically focused on patients admitted to a medical service, and we excluded patients admitted to an inpatient cardiology service, who may have more clear-cut cardiac etiologies of their troponin elevation, with more precise descriptive terminology used. We also did not adjudicate the provided diagnoses, and so we are unable to assess the accuracy of discharge diagnoses that are related to troponin terms. Additionally, our sample was from a single state and, while we included patients from several different types of hospitals across the state, our findings may not be generalizable to other regions of the country. Finally, our sample included patients with a limited age range which may also limit generalizability to other populations.
Conclusions
Our study highlights inconsistency in the terms used to describe elevated troponin levels in hospital discharge summaries, including no mention at all in a third of the sample. Given the prognostic value of troponin elevations, we recommend adoption of more precise language in hospital discharge summaries, specifically the terms outlined in the Fourth Universal Definition of MI consensus document. Use of these terms can help facilitate evaluation and management of these potentially higher risk patients after discharge. We hope that future clinical trials will illuminate the optimal management of myocardial injury and type 2 MIs.
Disclosures/Conflicts of Interest
The authors report nothing to disclose
Funding Information
Not applicable
Acknowledgements
Not applicable
Corresponding Author
Rebekah L. Gardner, MD
Associate Professor of Medicine
The Warren Alpert Medical School of Brown University
Rhode Island Hospital
593 Eddy Street, JB 0105
Providence, RI 02903
Email: rebekah_gardner@brown.edu
Phone: 401-444-8537
ORCID: 0000-0001-5823-9178