Background
Physician interaction with patients significantly impacts adherence and follow-through on medical plans. A large part of physician interaction with patients includes clinical education and guidance regarding specific medical conditions and treatments.1 Bedside rounding, in which the oral case presentation takes place in front of the patient at the bedside, has been previously identified as a way to collaborate with patients and identify areas for improvement regarding physician interaction.2,3 Bedside rounding has also been used to elicit and respond to patient views of interprofessional rounding.4,5 Alternatively, some physicians may regard bedside rounding as challenging due to lack of time, insufficient faculty experience, organizational constraints, lack of training, and decreased time-management efficiency with walk rounds and computerized charts.6 The literature has shown conflicting data. While some studies have shown improved patient satisfaction with bedside rounds,7–9 others have shown that patients may actually favor rounds outside the patient’s room.10–12
Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) is the first national, standardized, publicly reported survey of patient perspectives of hospital care. HCAHPS scoring is tied not only to hospital compensation but also an essential indicator of patient interactions.13 The basis for this study and intervention was from the HCAHPS survey, in which listening scores for physicians were identified as an area needing improvement. In the survey, physician listening is identified by the following questions:
-
Did your doctor treat you with courtesy and respect?
-
Did your doctor listen carefully?
-
Did your doctor explain your medical information in a way you could understand?
This study aimed to identify and implement a measurement tool to improve physician listening. We surveyed patients about their experience in the hospital, specifically regarding physician interaction. Subsequently, we implemented a standardized intervention at an inpatient medical service at an academic medical center. The overall goal was to increase the HCAPHS score by 1% in the first quarter of the fiscal year.
Methods
Patients admitted to the inpatient medical service at Rhode Island Hospital (Providence, RI) were surveyed during 2021 for this study. Rhode Island Hospital is a 720-bed acute care hospital in Providence, RI and is part of the Lifespan Corporation health care system. Bedside rounding was identified as the main intervention given previous evidence supporting improvements in patient experience. This was subsequently implemented on the teaching medicine service at Rhode Island Hospital.
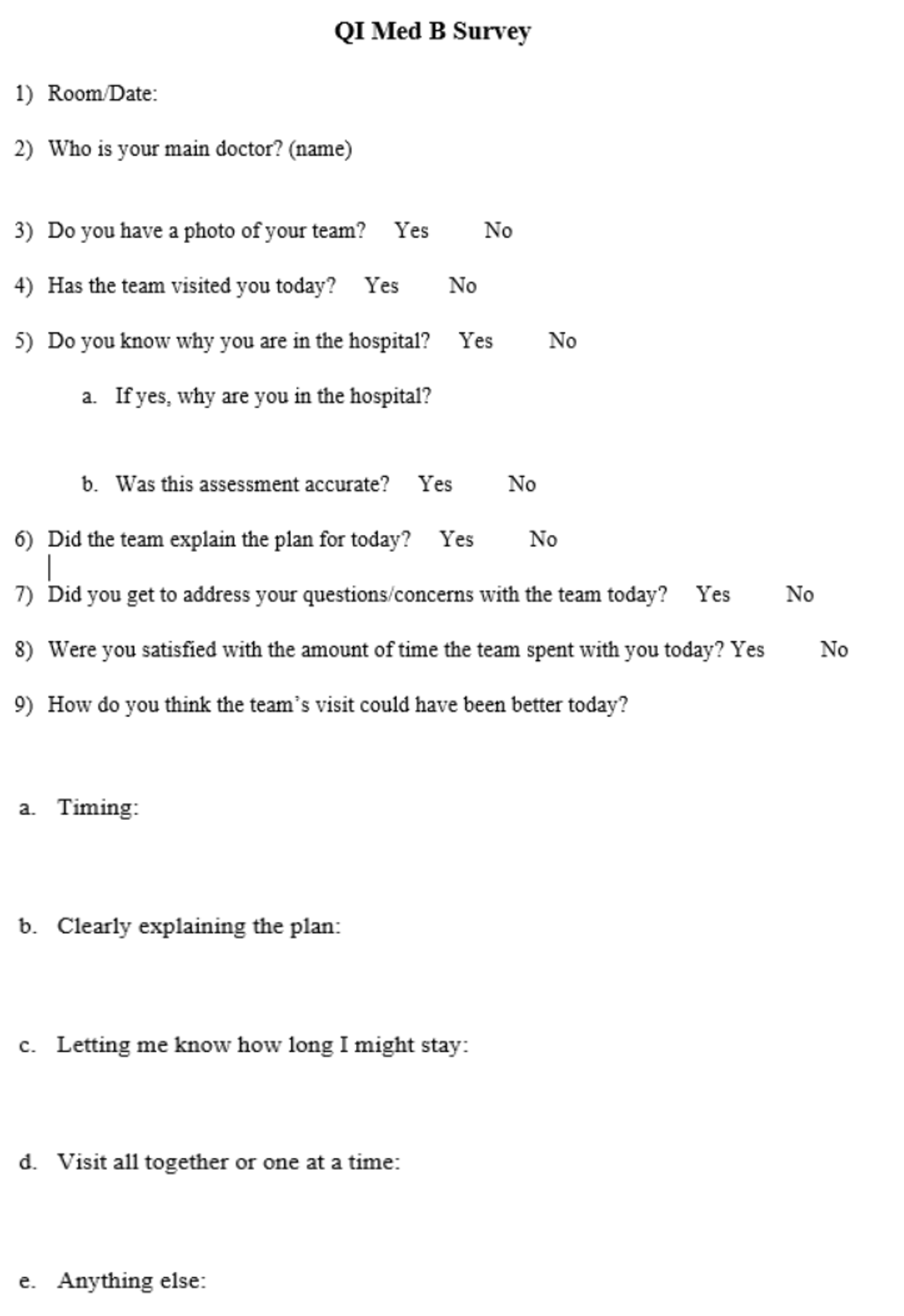
A standardized questionnaire was developed, and patients were surveyed at the outset prior to initiating bedside rounds. We educated internal medicine residents during didactic conferences to preface the intervention and present data. In addition, we performed a faculty staff meeting to discuss implementation of bedside rounding and feasibility. After coming to a consensus on the standardized bedside rounding process, we implemented the standardized bedside intervention. Figure 1 shows the survey tool that was developed for this study.

The standardized interventions included bedside rounding teams consisting of a teaching team on a geographic ward in the hospital. The team consisted of a teaching attending, a senior resident, interns, medical students, and, depending on the team, a pharmacist (to assist with medication reconciliation). The patients selected for team bedside rounding were identified at the senior resident’s or attending’s discretion. Patients with underlying medical conditions including dementia, aggressive or violent tendencies, or other behavioral disturbances or who were on contact and droplet precautions due to COVID-19 or other respiratory infections were often excluded. Roles of each team member were established upon entry into the patient’s room with a face sheet, and the intern was identified as the primary doctor for the duration of the hospitalization. The intern presented the plan while sitting at the bedside. The senior resident would place orders on the computer, facilitate communication with consultants and nursing, and update electronic handoffs. The patient presentation was a brief subjective, objective, assessment, and plan (SOAP) style format that was given using patient-centered language that minimized medical terminology. The plan was discussed at the bedside, with any further clarification sought from the attending physician. Teach-back methods were implemented after bedside rounding to ensure patient comprehension. On average, such rounding took approximately 5-15 minutes. Nursing presence was encouraged but not mandated at the bedside during this intervention due to staffing shortages due to the COVID-19 pandemic. After the study period (approximately one month), we performed a standardized survey to assess patient responses after the intervention of the standardized bedside rounding.
Results
A total of sixty-three patients were surveyed. Five teaching teams were asked to implement bedside rounding, each with an average census of 20 patients per team. Of the five teams, only three were able to perform bedside rounding.
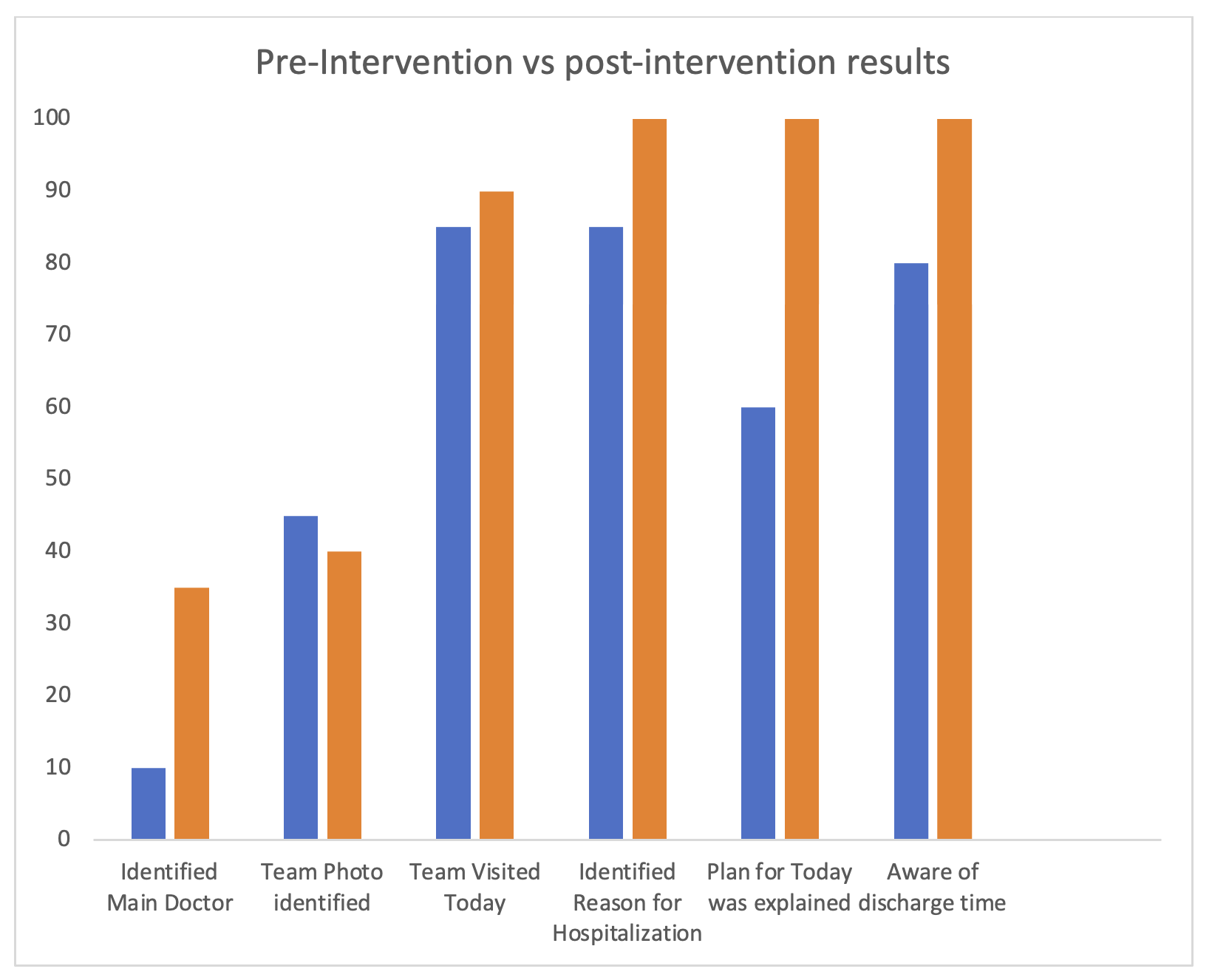
Initial survey results prior to the intervention demonstrated that only 60% of patients felt that the plan for the day was explained. And of patients who identified reason for hospitalization, 85% were accurate. 85% surveyed felt concerns were addressed on the day of interview. Approximately 78% were satisfied with amount of time team spent with them on day of survey.
After the intervention, 100% of patients surveyed felt that the plan for the day was explained. And of patients who identified reason for hospitalization, 100% were accurate. 100% surveyed felt concerns were addressed on the day of interview. Approximately 78% were satisfied with amount of time team spent with them on day of survey. Figure 2 shows the pre and post intervention results showing patient responses for the survey questionnaire categories.

Inter-group analysis was conducted using two sample T-test. This test compared groups post survey implementation between teams that implemented the intervention versus those who did not. Of the teams that were asked to implemented bedside rounding, only 50% were able to incorporate bedside rounding. A comparison of teams who performed bedside rounds versus those who did not perform bedside rounding using two sample T-test showed no that statistically significant differences were found between the two groups (Table 1).
Discussion and Conclusions
In this quality improvement initiative, standardized bedside rounding was used as a tool to improve patient-provider communication. Key results included a positive change in the patient identification of the reason for hospitalization and knowledge of the plan after implementing the standardized bedside rounding intervention. Analysis using a two-sample t-test revealed a p-value of 0.08 regarding the explanation of the plan between teams that implemented bedside rounding and those that did not fell short of statistical significance and showed no measurable change in patient knowledge.
A recent meta-analysis in the Journal of Patient Safety performed by Heip et al. was performed to determine the effect of interdisciplinary rounding on interprofessional communication and shared decision making.14 In this broad literature analysis bedside rounding was identified as potentially positively influencing patient-centeredness, quality of care, and team collaboration. However, definitive results remain uncertain due to variability in the quality of evidence, coordination challenges, and design. This continues to propel the need for further research in this field with more patient involvement in future studies.
The results of our initiative show some promise for implementing bedside rounds to improve physician listening and communication. Although the results of this study were not statistically significant, there was some improvement in findings that would impact patient outcomes in the future, such as identifying the reason for hospitalization and reason for hospitalization. The additional increase surrounding the knowledge of the medical plan (60% pre-implementation to 100% post-implementation) may in part have been due to more time spent in medical discussion at the bedside as an interdisciplinary team. Additionally, use of the teach back method as well as using patient centered language may have contributed to greater retention and understanding of the medical plan. In a more extensive study that is adequately powered, there may be a greater ability to identify differences between groups that perform versus do not perform bedside rounding.
Our study had many limitations. During the implementation process, internal medicine teams performed bedside rounding to varying degrees, as noted above. This may be due to the small sample size and population and variable implementation through the program. Typical factors cited by the teams’ included challenges regarding team turnover, patients being in contact isolation due to the COVID-19 pandemic, electronic medical record burden, and hesitation regarding presenting in front of patients at the bedside. Further, these results reflect data after only four weeks of implementation.
In conclusion, implementing a standardized bedside rounding initiative and survey methods showed a trend toward improved patient knowledge and physician listening as defined by HCAHPS. Prior studies have demonstrated a variable benefit of bedside rounding, with statistically significant improvements in patient experience but not in patient knowledge. In addition, it would be prudent to consider patient empowerment as a broader concept than just patient centeredness or patient participation.15 A longitudinal study with a larger population and an analysis after more consistent standardized implementation and patient surveying may yield significant results. Future directions could also compare HCAHPS scores in the listening category in teams that implement the standardized bedside rounding intervention vs. those teams who do not. Ultimately, more research needs to be performed to improve patient-centered outcomes around communication.
Acknowledgment
Lauren Young MD, Ibrahim Yusuf MD, Firrah Saeed MD, Belal Noureddine MD
Funding
No funding source to report
Conflicts of Interest
The authors have no conflicts of interest to disclose.
Corresponding author
Rasan K. Cherala MD
Brown University/Rhode Island Hospital Department of General Internal Medicine
593 Eddy Street, Providence, RI 02903
Email: rasan.cherala@gmail.com
ORCID: 0000-0001-5505-5840