Introduction
Lung abscesses are defined by the development of one or more cavities of necrotic debris with purulence in the lung parenchyma. Although most lung abscesses are treated with antibiotics, a lack of response to antibiotic therapy necessitates further interventions.1 Here we report the case of an adult immunocompetent patient with multiple lung abscesses managed with percutaneous drainage of the abscess and antibiotics.
Case Presentation
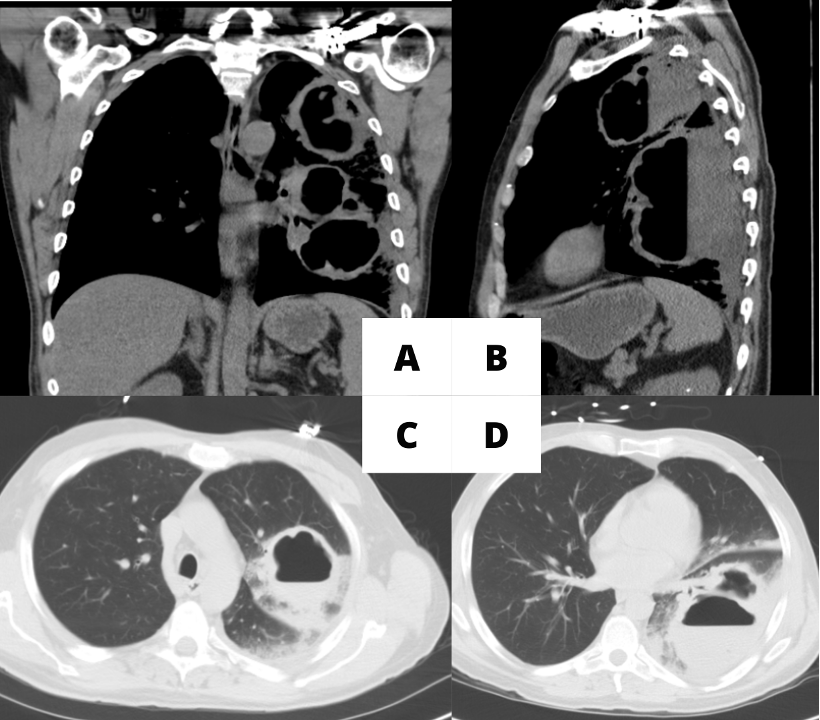
A 53-year-old male with a 35 pack-year smoking history, and alcohol use disorder, who presented with emesis and productive cough with dark colored sputum. On admission, the patient had a heart rate of 103 beats per minute. The respiratory clinical exam showed coarse upper airway sounds. C-reactive protein level was 325.2 mg/L and white blood count (WBC) was 20,000 upon admission. The chest computerized tomography (CT) showed two large lung abscesses with nodularity in the walls of the lung abscesses (Figure 1).
_at_the_time_of_admission._1-a_is_the_coronal_view_of_the_two_lung.png)
Infectious workup was negative for streptococcus urine antigen, legionella antigen, serum cryptococcal antigen, aspergillus galactomannan, histoplasma, blastomyces, coccidioides immitis antibodies and sputum acid-fast bacillus (AFB). HIV test was non-reactive, Quantiferon TB Gold was indeterminate. The echocardiogram did not show valvular vegetations, and panorex scan did not reveal dental caries. The initial sputum culture grew Klebsiella aerogenes.
Initial treatment with intravenous vancomycin and cefepime for one week failed to improve symptoms with patient suffering from persistent cough, recurrent fevers, and tachycardia. Hence percutaneous drainage of lung abscess was performed per recommendation of thoracic surgery consultants due to the size of the large size of both abscesses (>6 cm each) and persistent clinical findings of tachycardia, tachypnea, and leukocytosis.
The left upper lobe abscess was drained under CT fluoroscopic guidance. An 18-gauge Hawkins needle was used first, followed by the insertion of an Amplatz wire via the coaxial needle. It was replaced by a 10 French locking pigtail drain, after a series of tract dilation over the wire. 10ml of purulent fluid was drained and sent to microbiology for analysis. Similarly, the left lower lobe abscess was drained, and a pigtail drain was placed. Biopsy of the nodularity in abscess walls was performed using an 18-gauge biopsy needle and five samples were sent to pathology, to evaluate for possible underlying malignancy.
After drainage of the abscesses, the patient’s symptoms improved with the resolution of sepsis over the next two days. The results of the tissue analysis from the biopsy of the lung abscess wall showed marked acute inflammation, necrosis, and fibrinous exudate but were negative for malignancy. Gram stain and culture from abscess fluid showed polymorphonuclear white blood cells but no organism grew in the culture. Fungal and AFB cultures yielded no growth.
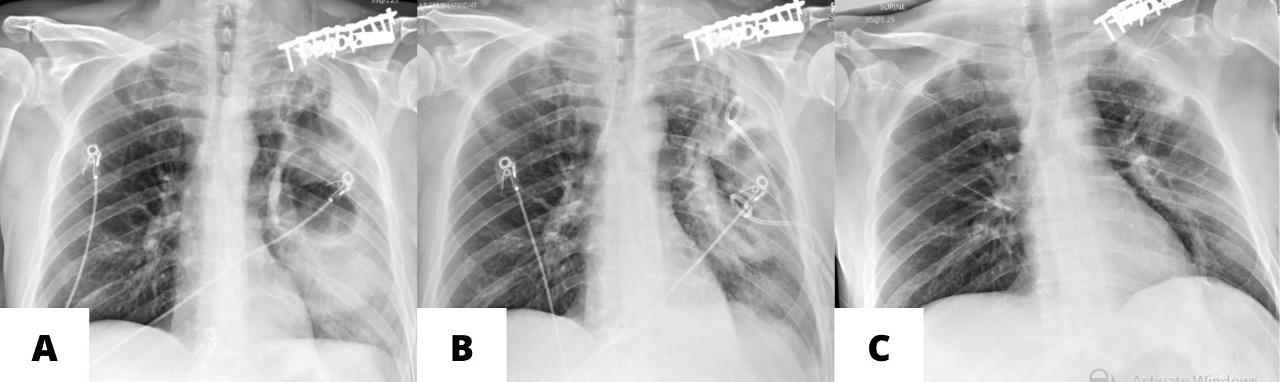
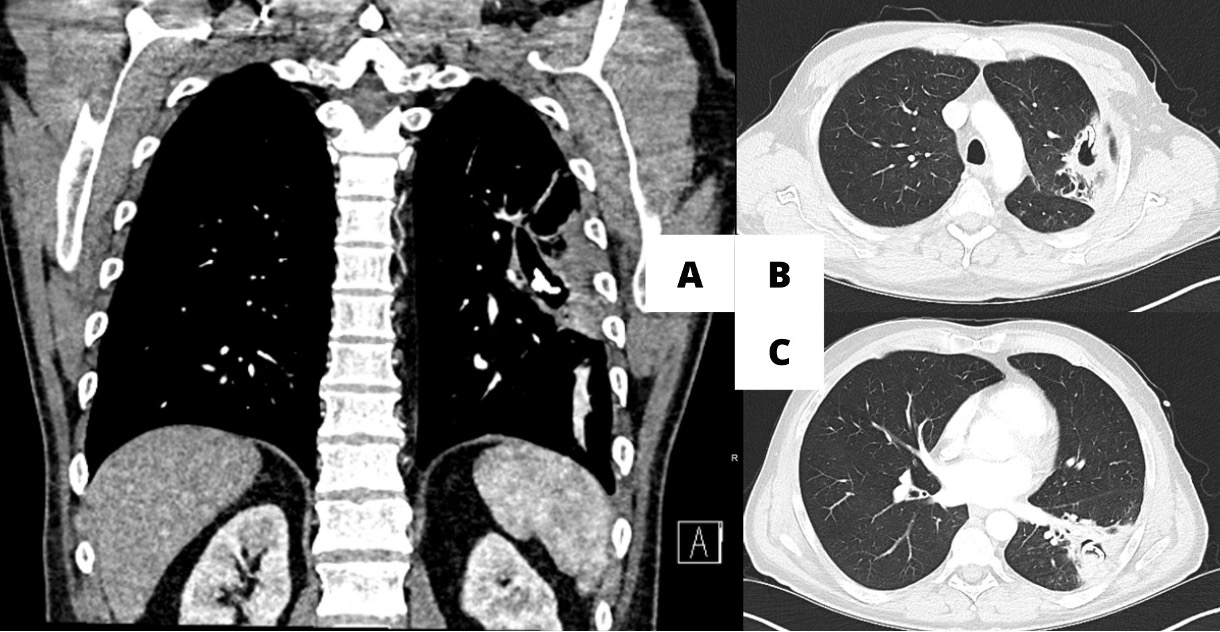
The patient was managed with levofloxacin and metronidazole for two weeks after the placement of drains, with the plan of continuing 4 more weeks of oral therapy after removal of the drains. Placement of drains resulted in a significant reduction (>50%) in the size of the cavities (Figure 2-B & Figure 3). CRP normalized to 1.3 mg/L and WBC was 4,000 at the time of discharge, with complete resolution of pulmonary symptoms.
__after_drain_placement_(2-b)__after_removal_of_.jpeg)

Discussion
Lung abscess is characterized by a bound area of necrotic debris or pus in the lung parenchyma that later forms a cavity. Lung abscesses are categorized as chronic when present for more than six weeks. They are also classified based on their etiology. Primary lung abscesses can be caused by immunodeficiency, aspiration of oropharyngeal secretions, or necrotizing pneumonia. Secondary lung abscesses can be caused by bronchial obstructions, malignancy, hematogenous seeding of infection, or direct dissemination.1 Management of lung abscess includes antibiotics, pulmonary physiotherapy, drainage, and pulmonary resection.1,2
Antibiotic therapy for bacterial lung abscesses is started empirically with beta-lactams (e.g., ampicillin-sulbactam) or carbapenems (e.g., meropenem) to target streptococci and anaerobes. Alternatively, moxifloxacin, clindamycin, or levofloxacin with metronidazole can be used in patients allergic to penicillin. Coverage for methicillin-resistant Staphylococcus Aureus (MRSA) and Pseudomonas are added based on the patient’s risk factors for the colonization of the respective organisms. Initial intravenous therapy is used until resolution of fevers and phlegm production then transitioned to oral antibiotic therapy to complete at least three weeks of antibiotic therapy or until a notable decrease in the size of the cavity on follow-up imaging.3
Although most lung abscesses are managed conservatively with antibiotics, in about 10%-20% of the patients, large size, persistent symptoms, and sepsis necessitate surgical intervention.4,5 Acute indications urging pulmonary resection include hemoptysis, prolonged sepsis, and bronchopleural fistula. Chronic indications include persistent pulmonary symptoms, cavitations larger than 6 cm, and infections unresponsive to antibiotic treatment for greater than six weeks.2 The pathogen’s virulence, inability to achieve necessary antibiotic concentration in the abscess cavity, and advanced lung disease are some reasons for the failure of antibiotic therapy.4 An alternative to the pulmonary resection is percutaneous drainage under radiographic guidance, as seen in this case. This minimally invasive technique can be implemented in medium to high-risk patients who are poor candidates for surgical resection.2,4 It also avoids potential complications associated with surgery; moreover, percutaneous drainage reduces the need for secondary surgical intervention. Percutaneous drainage has an overall lower mortality rate at 4% and higher efficacy.4,6 Possible complications of percutaneous drainage include pain at the drain site, obstruction and dislodgement of the drain, pneumothorax, hemothorax, hemoptysis, pleural contamination leading to empyema, and development of bronchopleural fistula.2
Although it has high efficacy and success rates, the procedure is still disputed as the standard of management of large lung abscesses. It is not always favorable in the setting of virulent pathogens, multi-loculated abscesses, with poor visualization of the cavity, thick-walled cavity, or secondary lung abscess.4 In this case, it is evident that the drainage coupled with antibiotic treatment was successful despite the two large-sized abscesses. Aspiration in the setting of alcohol abuse was the suspected cause of the lung abscesses in the above case. In summary, this is an unusual case of multiple, large lung abscesses that did not respond to antibiotic treatment initially and were drained by CT fluoroscopy-guided percutaneous drainage and spared the patient from surgery.
Funding
None
Conflict of Interest
The authors have no conflicts of interest to disclose.
Author Contribution
All Authors (PJ, HT, SA) have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding Author
Perla Carolina Jorge, MD
Department of Radiology, Massachusetts General Hospital, Harvard University, 25 New Chardon St., Suite 501
Boston, MA 02114
Email: pjorge@mgh.harvard.edu