Background
Valproate is a commonly used medication as an antiepileptic and mood stabilizer. A retrospective cohort study evaluating critically ill adults treated with valproate for agitation showed a reduction in agitation, delirium, and concomitant psychoactive medication use within 48 hours of initiation.1 This was confirmed later by another retrospective descriptive analysis.2 The 2018 Society of Critical Care Medicine guidelines address valproate’s role in managing agitated delirium.3 Valproate may have a role in managing hyperactive delirium if antipsychotic drugs have failed or are contraindicated, e.g., prolonged QT or extrapyramidal symptoms, and dexmedetomidine cannot be used, e.g., adverse cardiovascular effects. However, the same guidelines address the lack of evidence and the need for rigorous studies to address safety and efficacy.3 Hypoperfusion and dysphagia frequently complicate medical illness in geriatric patients. Organ injury associated with hypoperfusion commonly involves the kidneys, brain, bowel, liver, and rarely, the esophagus. We describe an elderly male who presented with COVID-19 infection, hyperactive delirium, acute kidney injury, and hypotension, and developed acute pancreatitis secondary to valproate therapy along with acute esophageal necrosis.
Case Presentation
76-year-old male with a past medical history of hypertension, stage 4 severe chronic kidney disease, gastroesophageal reflux disease (GERD), and depression presented with a one-week history of altered mental status. His home medications included amlodipine, hydralazine, isosorbide mononitrate, and sertraline. Vital signs at the time of admission were normal. Physical exam showed orientation limited only to self with signs of dehydration. The neurological exam was limited by poor cooperation but showed intact motor function. The laboratory analysis noted an elevated serum creatinine level of 4 mg/dl from a baseline of 2 mg/dl. Magnetic resonance imaging (MRI) of the brain and computed tomography (CT) head were unremarkable. Chest CT scan showed right lower lobe consolidation. He tested positive for COVID-19 infection and was isolated.
The patient did not require supplemental oxygen throughout his stay. Due to renal impairment, he was not treated with remdesivir or baricitinib. Worsening of renal function and metabolic acidosis necessitated the initiation of hemodialysis. His blood pressure did not tolerate initiation of hemodialysis with intermittent hypotension as low as 90 mmHg systolic blood pressure (SBP). These episodes were largely responsive to intravenous fluid challenges and discontinuation of hydralazine, isosorbide mononitrate, and amlodipine.
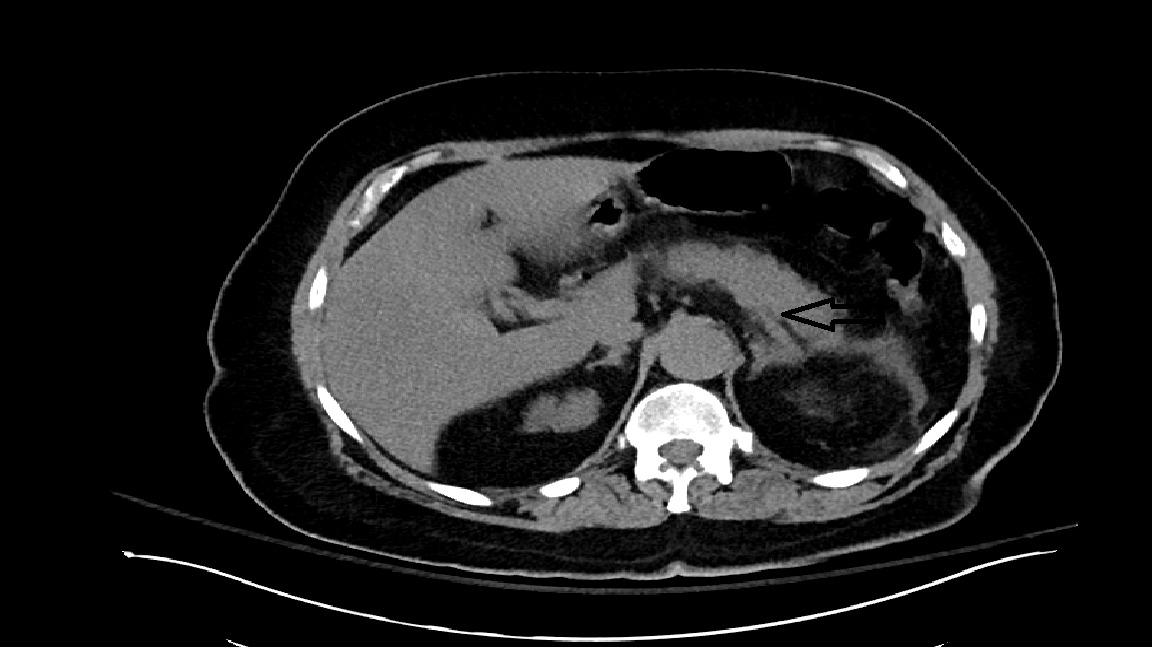
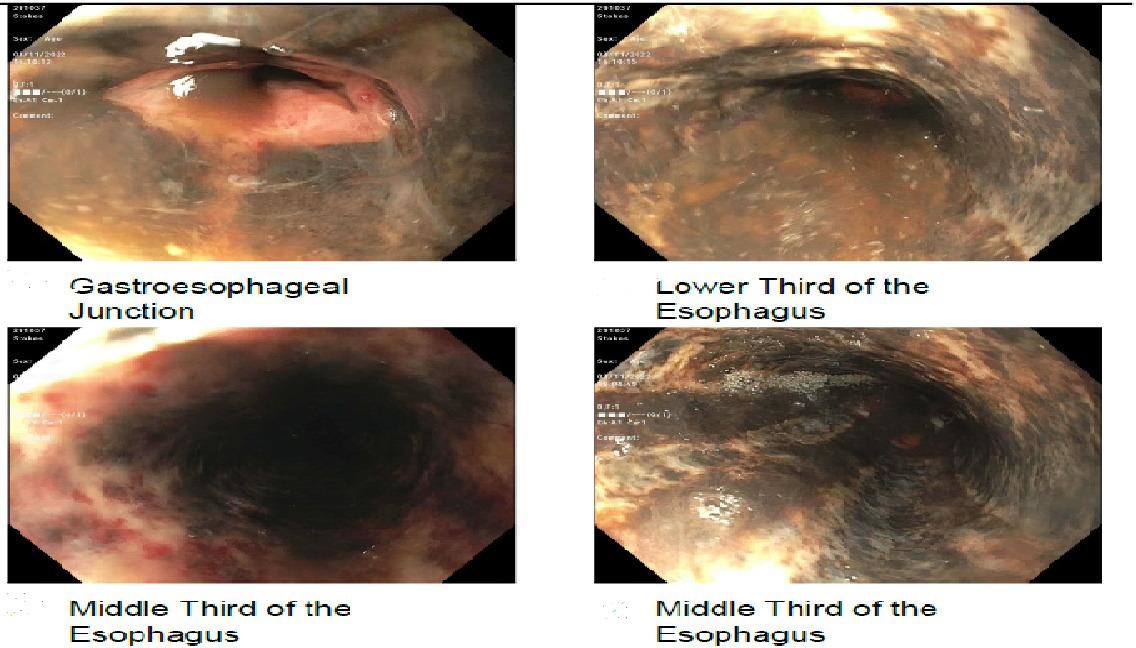
He remained confused and agitated and was diagnosed with progressively hyperactive delirium. Antipsychotic medications, including trazodone and quetiapine, were added without adequate symptom control. Valproate was added and maintained at 250 mg twice daily with a serum level of 41 mcg/mL (reference range 50-99 mcg/mL). He was noted to have poor oral intake and new onset dysphagia to both solids and liquids. He developed hematemesis with elevated lactic acid above 5 mg/dL. His physical exam was significant for epigastric tenderness. CT of the abdomen with intravenous contrast ruled out intestinal ischemia, but acute pancreatitis was suggested by pancreatic stranding and confirmed by elevated serum lipase above 5000 U/L (Figure 1). Valproate was held 17 days after its initiation. Acute pancreatitis was treated supportively with an improvement of serum lipase. EGD revealed severe diffuse ulcerative esophagitis, circumferential submucosal hemorrhages, and gangrenous changes suggestive of ischemic injury (Figure 2). Infusions of proton pump inhibitor (PPI) and peripheral partial nutrition (PPN) were initiated. However, the patient continued to deteriorate clinically with a further decline in hemoglobin level, hypotension, and hypothermia.
_scan_of_the_abdomen_showing_stranding_of_the_pancreas_suggestive_.png)
_showing_diffuse_gangrenous_discoloration_of_the_esophagus.jpeg)
His overall prognosis was deemed poor, and goals of care discussions concluded in pursuing comfort measures.
Discussion
Pancreatitis due to valproate is rare, and only around 120 cases have been published in medical literature, including several fatal cases. The incidence of valproate-induced pancreatitis has been estimated to be 1:40,000. It has been more commonly reported in children and young people.4 Our case shows this complication occurring in an older adult. Pancreatitis due to valproate has been reported as a dose-dependent reaction and idiosyncratic side effect. There is no established association between the dosage or serum valproate level with its development.5 The patient had other risk factors of pancreatitis, including chronic renal failure and episodic hypotension. However, improvement and eventual normalization of lipase after discontinuation of valproate suggest it was likely a drug-induced reaction.
The Naranjo score is used to assess the probability of a drug-induced reaction. Given the previous conclusive reports of valproate-induced pancreatitis, temporal relationship after starting valproate, significantly elevated lipase, improvement of pancreatitis after discontinuation of valproate, and lack of other significant etiologies, the calculated Naranjo score was seven, which indicates the likelihood of drug-induced pancreatitis in this case.6
Acute esophageal necrosis (AEN), commonly referred to as “black esophagus” or “acute necrotizing esophagitis,” is a rare clinical disorder characterized by a striking endoscopic image of diffuse, circumferential, black-appearing, distal esophageal mucosa on EGD that stops abruptly at the gastroesophageal junction.7 AEN occurs when normal esophageal defensive mechanisms are impaired by factors like diabetes, renal failure, immunosuppression with acute decline in blood supply in the setting of sepsis, severe pancreatitis, lactic acidosis, and diabetic ketoacidosis. Typically reported in patients with hemodynamic shock, cases have also been reported in the setting of a transient low-flow state associated with a combination of different antihypertensives.8 Further injury to the esophagus is induced by reflux esophagitis. This is commonly referred to as the two-hit hypothesis. Antibiotics have been noted to play a role in the development of AEN.9 We suspect that atherosclerotic vascular disease may have predisposed our patient to AEN. Those with underlying established atherosclerosis, e.g., stroke and coronary artery disease or risk factors including diabetes and hypertension, have a higher risk for AEN. Once suspected, the diagnosis can be confirmed by EGD. Management is mainly supportive with intravenous fluids, nil per os (NPO) status, and proton pump inhibitors.
The association between COVID-19 and acute pancreatitis is poorly defined. Up to 17% of patients with severe COVID-19 have pancreatic injury with high serum lipase and amylase levels, while 7% had imaging findings compatible with pancreatitis.10 A recent systematic review concluded that there is insufficient evidence showing that COVID-19 can cause pancreatitis or negatively impact prognosis.11 Recently, a case was reported of AEN in a COVID-19 patient with the suggestion that COVID-19-related prothrombotic state and hypoperfusion contributed to its development.12
In conclusion, AEN or “black esophagus” is a marker of poor prognosis that is hypothesized to be related to hypoperfusion and reflex injury of the esophagus. AEN should be suspected in those with new-onset dysphagia and poor oral intake due to predisposing risk factors. Valproate-induced acute pancreatitis is a rare but known adverse effect. Clinicians must be aware of this complication in order to diagnose this condition in a timely fashion and prevent complications.
Disclosures/Conflicts of Interest
The authors of this paper have no disclosures.
Author Contribution
All Authors (MAA, OA, DG) have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
• Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
• Drafting the work or revising it critically for important intellectual content; AND
• Final approval of the version to be published; AND
• Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding Author
Mohammad Abu-Abaa, MD
Capital Health Regional Medical Center Internal Medicine Residency Program 750 Brunswick Ave, Trenton, NJ
Email: Mabu-abaa@capitalhealth.org
ORCID ID 0000-0003-1752-1235