Introduction
Hypertensive emergency is defined as an elevation in blood pressure, usually greater than 180/110-120 mmHg, with evidence of acute target-organ damage. An estimated 4.6% of all emergency room visits are due to acute severe hypertension.1 Manifestations of acute target-organ damage include acute kidney injury, acute heart failure, acute coronary syndrome, aortic dissection, stroke, hypertensive encephalopathy, and papilledema. Therefore, blood pressure control must be achieved promptly to avoid life-threatening complications.1 The etiology of hypertension is diverse and includes rare causes of common organ system diseases, which calls for a more nuanced approach to dealing with the condition. We describe a patient with a hypertensive emergency in the setting of chronic kidney disease due to a very rare genetic disorder called UMOD-Related Autosomal Dominant Tubulointerstitial Kidney Disease (ADTKD-UMOD). This case illustrates the difficulty of designing an adequate blood pressure management therapy for a rare genetic disease causing long-standing resistant hypertension.
Case Presentation
A 39-year-old man with a past medical history of hypertension, gout, hyperlipidemia, gastroesophageal reflux disease, and chronic kidney disease stage IV secondary to ADTKD-UMOD presented to the emergency department (ED) with shortness of breath, cough, and new onset chest pain. Over the past month, he had episodic shortness of breath, sometimes associated with frothy white sputum. The symptoms gradually worsened until one morning, he felt chest pain like never before, and his nephrologist advised him to report directly to the hospital. ADTKD-UMOD was previously diagnosed through genetic testing after the patient had his first gouty attack at 17. Surgical history was notable for right upper extremity repair following a chainsaw injury. Family and social history were unremarkable. Given the autosomal dominant nature of ADTKD-UMOD, this was surprising to us, but the patient reiterated that he knew of no known medical problems in his immediate family. This was confirmed upon 1-month follow-up. The patient reported no known allergies, and his home medications consisted of clonidine, carvedilol, febuxostat, atorvastatin, and famotidine.
Upon evaluation in the emergency department, initial vital signs were significant for blood pressure 168/117 mmHg. The physical exam was significant for basilar crackles, non-pitting lower extremity edema, frothy sputum production, and non-palpatory/non-pleuritic left-sided chest pain. Initial labs revealed a blood urea nitrogen (BUN)/serum creatinine (Cr) of 49.8/4.56 mg/dL (BUN ref 6 to 24 mg/dL; Cr ref 0.7 to 1.3 mg/dL) with a known baseline Cr in the range of 3.1 to 3.3 mg/dL. His ED course was further complicated by an acute rise in his blood pressure of 219/166 mmHg and a decreased SpO2 of 93%, which responded promptly to 4 liters of supplemental oxygen. High-sensitivity serum troponin levels were elevated at 111 ng/mL (ref <14ng/L) without a change at three hours. B-type natriuretic peptide (BNP) was elevated at 715 pg/mL (ref <100pg/mL), and uric acid level was 8.6 mg/dL (ref 3.5 to 7.2 mg/dL). Urinalysis on admission showed proteinuria of 300 mg/dL (ref 0 to 14 mg/dL). The table shows trends of his BUN/Cr and blood pressure during his hospital course.
The diagnosis of hypertensive emergency was made given that the acute elevation in blood pressure had led to acute kidney injury and elevated levels of cardiac biomarkers and BNP suggestive of acute myocardial injury/ischemia. Management in the emergency department consisted of IV hydralazine, IV labetalol, and clonidine by mouth. This regimen improved his blood pressure to 180s/120s mmHg. He was admitted to the inpatient medicine service to titrate his blood pressure medications and manage acute kidney injury.
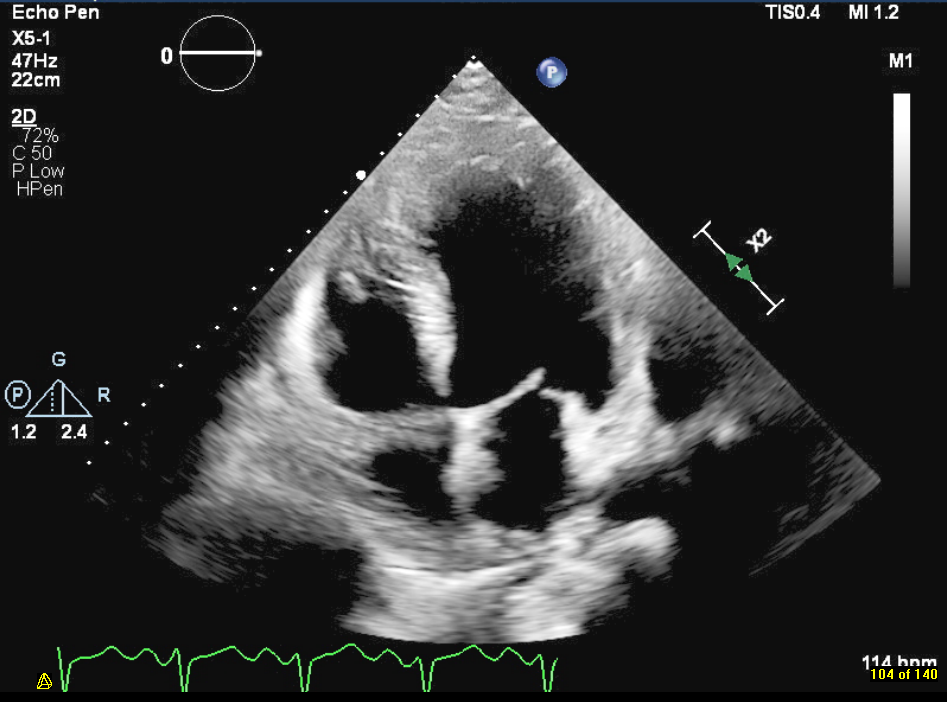
During hospitalization, the patient got a renal ultrasound showing bilateral echogenic kidneys without hydronephrosis. Transthoracic echocardiogram, shown in Figure 1, revealed a left-ventricular ejection fraction of 15-20% with severe global hypokinesis of the left ventricle. He was started on a regimen of hydralazine 50 mg daily, a nitroglycerin patch, and furosemide 40 mg IV once daily. Once he tolerated the nitroglycerin patch without significant side effects, he was switched to combination isosorbide dinitrate/hydralazine. His kidney function stabilized over the preceding days, and he responded well to therapy. Prior to discharge, doxazosin was added for better control of blood pressure. After five days of hospitalization, the patient was discharged with a blood pressure range of 139-163/97-102 mmHg. Furosemide may provide a potential benefit in ADTKD-UMOD, but the patient’s renal function deteriorated significantly during the hospital stay. Furosemide was ultimately withdrawn in hopes of preserving renal function after a collaborative discussion between the cardiologist, nephrologist, and the primary team. His blood pressure medication regimen on discharge was carvedilol 25 mg twice a day, hydralazine-isosorbide dinitrate 37.5 mg/20 mg twice a day (to be up-titrated as an outpatient), and doxazosin 4 mg once a day.
_revealing_ef_of_15-20___global_hypokinesis_o.png)
One month after hospitalization, the patient has recovered well and is back to his job as a police officer. His symptoms have improved, and his blood pressure is better controlled, averaging 135/90-100 mmHg. The patient is being evaluated for renal trasplantation, but further evaluation requires his left ventricular ejection fraction to improve to greater than 40%. He has returned to his normal daily living activities, and is followed closely by his nephrologist and cardiologist.
Discussion
Patients who develop a hypertensive emergency are at risk of worsening target-organ damage, so it is critical to lower blood pressure safely and timely. Current guidelines for lowering blood pressure during an acute hypertensive emergency recommend lowering blood pressure by 20-25% in the first hour and to 160/100 mmHg with 2-6 hours.1 The use of IV hydralazine is associated with significant concerns related to an unpredictable and often excessive blood pressure reduction, tachycardia, and potential worsening of myocardial ischemia.1 This risk was mitigated to some extent by using a beta blocker like carvedilol, which this patient was already taking.
ADTKD-UMOD, caused by a rare mutation in the UMOD gene, is a storage disorder of the endoplasmic reticulum, which results in chronic kidney disease due to the deposition of abnormal uromodulin over time in the thick ascending limb. The function of uromodulin (aka Tamm Horsfall glycoprotein) is still unknown. However, it likely is responsible for maintaining the integrity of the thick ascending limb with positive regulation of the NKCC2 transporter.2 In fact, UMOD risk variants associated with higher uromodulin levels and activation of NKCC2 are theorized to have a stronger response to furosemide; however, research in this domain is ongoing.3 The risk allele, while favoring salt retention, has been theorized to be kept at high population frequency because high uromodulin levels in the urine likely protect against UTIs.2 Once uromodulin is mutated, however, NaCl reabsorption reduces, and the body forms a state of volume contraction known to promote the proximal reabsorption of urate, leading to hyperuricemia.4
ADTKD-UMOD accounts only for approximately 0.2% of individuals with end-stage renal disease (ESRD), with 2000 recognized cases in 2020.5 In genome-wide association studies, UMOD alleles associated with higher uromodulin expression were associated with increased risk of CKD and hypertension but was shown to be protective against kidney stones.3 Clinical features typically include nocturia in children, progressive loss of kidney function, bland urinary sediment, and normal/small kidneys on ultrasound. Laboratory findings include hyperuricemia, low fractional excretion of urate, and low urinary excretion of uromodulin.5 Patients often have no history of arterial hypertension preceding the onset of impaired kidney function. With progressive disease, blood pressure usually increases modestly. In patients without kidney disease, lowering uric acid levels led to clinically significant improvements in lowering blood pressure.5 Some patients may develop a renal phenotype consisting of, but not limited to, arteriosclerosis, glomerular hypertension, glomerulosclerosis, interstitial disease, and acute kidney injury.6 With time, patients with this condition are at high risk of developing a hypertensive emergency.
ADTKD-UMOD confers a 50% lifetime risk of developing gout (hypouricosuric hyperuricemia).7 The mechanisms behind hyperuricemia precipitating hypertension can be explained by activation of the renin-angiotensin-aldosterone system, stimulation of NADPH oxidase, and low endothelial nitric oxide synthase/nitric oxide availability. This, in turn, exacerbates renal vasoconstriction, oxidative stress, and ischemia. In the long-term, immune cell activation occurs in the kidney in response to these changes, leading to salt-sensitive hypertension.8 Furthermore, increased uric acid levels, whether by increased production or decreased excretion, can lead to activation of mitogen-activated protein kinases (MAPK) and stimulation of NADPH oxidase that triggers oxidative stress in the mitochondria and cytoplasm. This oxidative stress activates inflammatory pathways in multiple types of cells, including vascular endothelial cells.8 To give an example, in an eight-week double-blind crossover study, allopurinol was found to reduce blood pressure in adolescents with newly diagnosed hypertension with an associated drop in systemic vascular resistance and renin activity.8 However, studies evaluating the effect of urate-lowering therapy in patients with chronic kidney disease have found minimal to no improvement in blood pressure. The reason may relate to immune mechanisms becoming dominant in driving hypertension in subjects with kidney disease, with hyperuricemia no longer the main culprit.8 In patients with ADTKD-UMOD, allopurinol treatment appears to be beneficial for controlling symptoms but has not been shown to decrease disease progression.7
This case illustrates the difficulty of managing patients with many forms of genetic kidney pathologies. Nearly 70 mutations in the UMOD gene have been discovered worldwide, many within exons 3 and 4 of the UMOD gene. Among Caucasian patients, the average age of onset of hyperuricemia and ESRD was 24 and 56 years, respectively.9 In a randomized cohort of 3315 patients, exome sequencing yielded a genetic chronic kidney disease diagnosis in just under 10% of cases. Among those, only 3% yielded a mutation in the UMOD gene.10 The study’s findings support the diagnostic utility of exome sequencing to accurately direct patients to relevant clinical trials and targeted therapies. 95.3% of UMOD mutations that resulted in ADTKD-UMOD were found to be missense mutations. Due to these missense mutations, mutated uromodulin produced non-functional proteins and uromodulin aggregates within the endoplasmic reticulum that led to apoptosis.3,11 This mechanism suggests that using antisense oligonucleotides may be a strategy to slow disease progression.3 Moreover, the male gender was a significant predictor of worse renal outcomes.12 Onset of ESRD was significantly earlier in patients with mutations in the epidermal growth factor domains of the UMOD allele (45-52 years) than in the cysteine-rich domains (60-65 years).12
It is important to emphasize that the blood pressure regimen offered was only a temporary measure to address the natural progression of ADTKD-UMOD. Diuretics should be used cautiously in patients with ADTKD-UMOD, as they may aggravate hyperuricemia and volume depletion.5 Other patients with this genetic disease progressed to requiring dialysis between 18-52 years old.7 Our patient was already in discussions with his nephrologist regarding renal replacement therapy before progressing to end-stage renal disease (ESRD). Ultimately, renal transplantation is the only cure for this condition.4 Individuals with ADTKD-UMOD are excellent transplant candidates due to the slow progression of the disease allowing time to find a living donor. If the patient develops ESRD before a transplant, renal replacement therapy such as hemodialysis or peritoneal dialysis are potential options.4
In conclusion, this case of hypertensive emergency in a patient with a rare etiology of chronic kidney disease demonstrates the nuance of tailoring therapy for common conditions with uncommon etiologies. The key initial step to managing hypertensive emergencies is recognizing the risk to target organs. The optimal therapeutic approach necessitates understanding the patient, their symptoms, and comorbid conditions to tailor a regimen best suited for the clinical situation.
Acknowledgements
I would like to acknowledge Dr. Zeel Patel in assisting with editing and providing feedback. Thank you to Dr. Qaisra Saeed for providing echocardiogram images.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Author Contribution
All Authors (TC, SS) have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
- Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
- Drafting the work or revising it critically for important intellectual content; AND
- Final approval of the version to be published; AND
- Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.