Background
Pneumonitis related to immune checkpoint inhibitor (ICI) therapy is a widely recognized immune-related adverse event that can occur during the treatment of various malignancies.1 Immune checkpoint inhibitor pneumonitis can be fatal, and prompt diagnosis and treatment are crucial.2 While ICI pneumonitis has been widely reported to cause bilateral multifocal pulmonary infiltrates, unilateral pneumonitis has been reported only twice prior, and associated pneumothorax has only rarely been reported.3–5
Case Presentation
A man in his 80s presented with three sites of subcutaneous nodules and a left upper lobe lung nodule related to metastatic melanoma. Genetic analysis of tumor tissue revealed no evidence of BRAF and NRAS gene mutations, and an activating mutation in c-KIT gene was found. Medical history was remarkable only for a remote 9 pack-year smoking history. He was treated with pembrolizumab 200 mg monotherapy every 21 days and had a complete response after 3 cycles. He reported no prior adverse events from pembrolizumab.
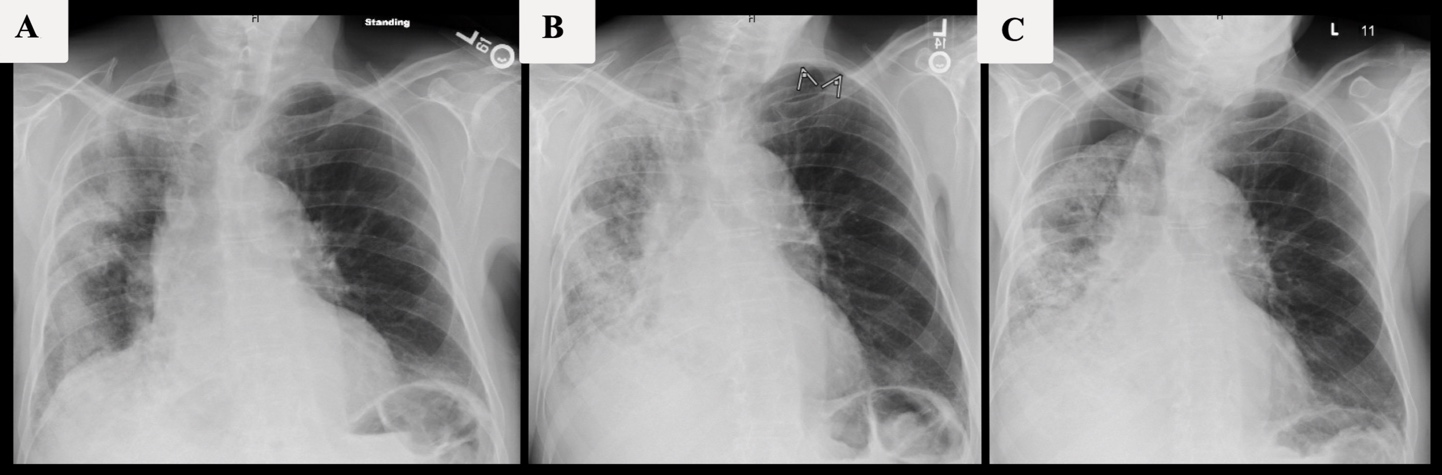
Three days after receiving cycle 7 of pembrolizumab, he presented to the hospital with worsening dyspnea on exertion and dry cough exacerbated when supine and on his right side. He denied fever, rigors, and sputum production. Vital signs were within normal limits including oxygen saturation while breathing ambient air. His physical examination was remarkable for rales at the right lung base, trace lower extremity edema midway up the shins bilaterally, and jugular venous pressure elevated to the mandibular angle with the head of the bed at 45-degrees. A chest x-ray (CXR) showed unilateral, patchy airspace opacities involving all three right lung lobes (Figure 1A). High-sensitivity serum C-reactive protein (CRP) was elevated to 183.5 mg/L; serum procalcitonin (0.08 ng/mL) and white blood cell count (9,300 cells per microliter) were within normal limits. Two sets of blood cultures were negative. He was empirically treated for community-acquired pneumonia (CAP) with a 5-day course of cefuroxime and doxycycline with improvement of symptoms. He was given furosemide for peripheral edema and an elevated serum B-type natriuretic peptide level of 5,821 pg/mL (reference range: <450 pg/mL). An echocardiogram demonstrated normal left ventricular systolic and diastolic function, moderate mitral regurgitation, and mild aortic stenosis.
_with_progressive_pleural_effusion_and_unilateral_o.jpeg)
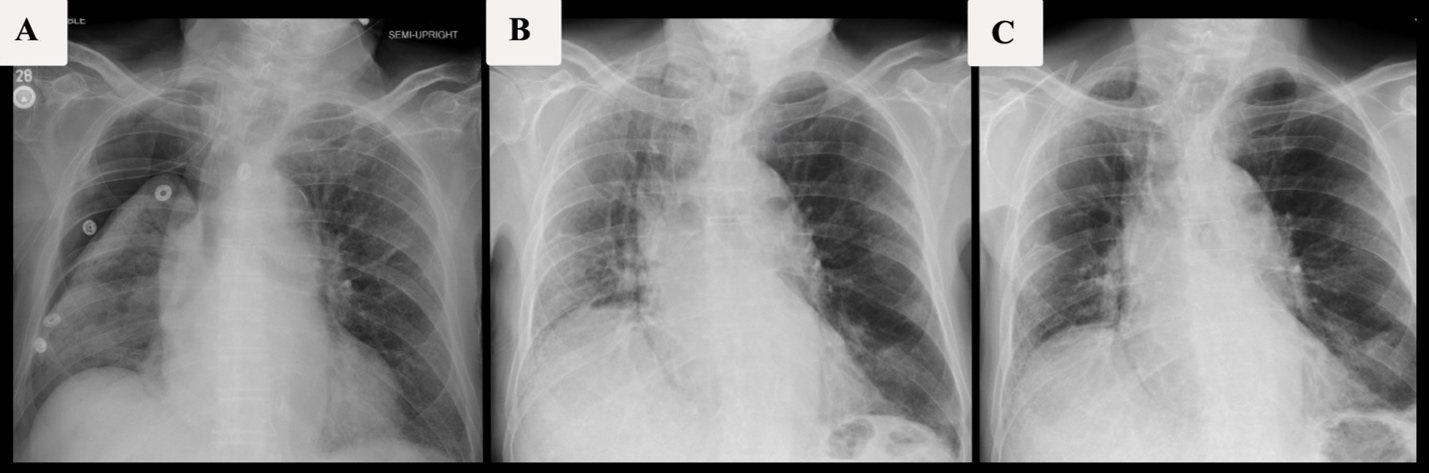
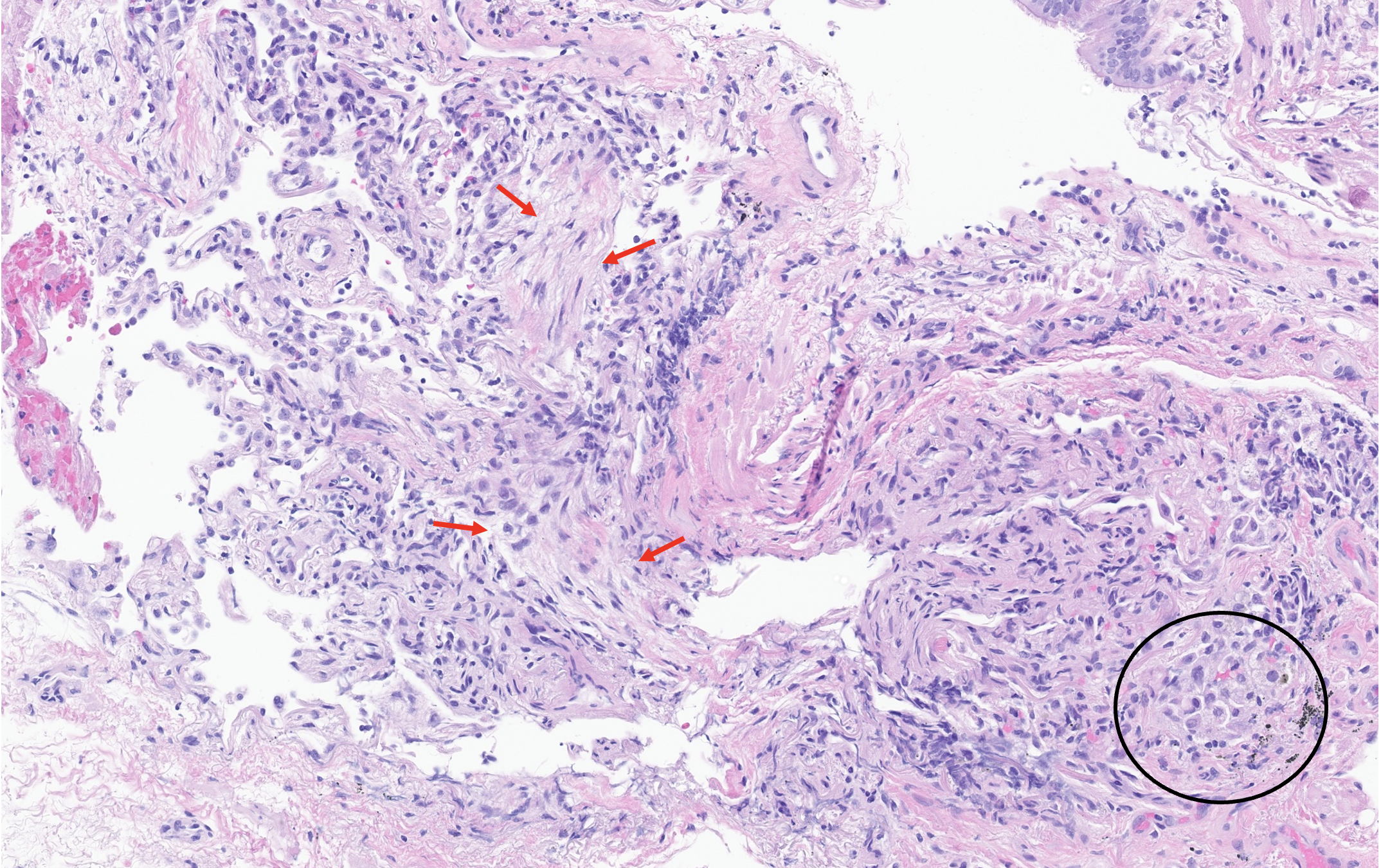
Eighteen days after discharge, he presented to oncology clinic with recurrence of dyspnea and cough. A pleural effusion and interval increase in the right-sided lung opacities were found on CXR (Figure 1B), and he was prescribed a 5-day course of levofloxacin for CAP. His symptoms persisted, and, on day 5 of levofloxacin, he was readmitted to the hospital after a repeat CXR demonstrated a right-sided hydropneumothorax (Figure 1C). He continued to have normal vital signs and oxygen saturation, and his physical exam demonstrated coarse crackles throughout the right-sided posterior chest fields. A chest tube was placed (Figure 2A) with pleural fluid analysis showing >15,000 nucleated cells per microliter, 48% granulocytes, 5% lymphocytes, and 2% eosinophils. Although the right lung re-expanded on subsequent CXRs, he had persistent right-sided lung opacification and dyspnea on exertion after 3 days of broad spectrum antimicrobial therapy, which led to bronchoalveolar lavage (BAL) and transbronchial biopsy. BAL showed 435 nucleated cells per microliter with 73% lymphocytes, 11% granulocytes, and 2% eosinophils. No malignant cells or organisms were demonstrated in either pleural or BAL fluid. Transbronchial biopsy of the right middle lobe demonstrated minimal inflammatory changes of the interstitium and airways and a possible focus of fibroblastic tissue consistent with organizing pneumonia (Figure 3).
__13_days_after_prednisone_in.jpeg)
__slight_prominence_of_pn.png)
The chest tube was removed shortly after, and he was discharged from the hospital while taking prednisone 60 mg per day for the treatment of ICI pneumonitis. Serial CXR films taken 13 and 22 days after initiation of corticosteroid treatment demonstrated continued improvement, and prednisone was tapered to 40 mg on day 13 and 30 mg on day 22 with improvement of symptoms (Figure 2B, 2C). Despite this clinical and radiographic improvement, the patient unexpectedly died of other causes near the end of the prednisone taper course. He was never rechallenged with pembrolizumab.
Discussion
ICI pneumonitis, defined as focal or diffuse lung parenchymal inflammation, has an estimated incidence rate of 2 to 5% and can occur at any time during immunotherapy, as demonstrated in this case with onset of symptoms after 6 cycles of pembrolizumab.1,6 Common presenting symptoms include dyspnea (53%) and cough (35%), both of which were seen in this case.1 Notably, fever (12%) and chest pain (7%) are less common.1 The median time to onset of ICI pneumonitis is estimated to be 2.8 months.1 Risk factors associated with ICI pneumonitis include age less than 60 years, high body mass index, male sex, smoking, and pre-existing interstitial lung disease.7 Other than a remote smoking history, our patient did not have any recognized risk factors for ICI pneumonitis.
In addition to diversity in the temporality of ICI pneumonitis’ presentation, there is also diversity in the radiographic presentation. On chest computed tomography (CT) scans, radiographic findings similar to organizing pneumonia, nonspecific interstitial pneumonia, hypersensitivity pneumonia, acute interstitial pneumonia, and sarcoid-like granulomatosis have all been described.6 One group stratified ICI pneumonitis into early- and late-onset subtypes in order to study potential clinical and radiographic differences.6 Patients with early-onset ICI pneumonitis (within 6 weeks of therapy) had more severe symptoms, poorer prognosis, and, more frequently, an organizing pneumonia-like radiographic pattern.6 In contrast, patients with late-onset ICI pneumonitis (>6 weeks of therapy) had fewer symptoms, better prognosis, and NSIP-like findings as the dominant radiographic pattern.6 Histopathologic findings in ICI pneumonitis are not as well characterized as the radiographic features. The most common reported pathologic finding is organizing pneumonia, followed by other non-specific inflammatory changes such as vague airspace granulomas, foamy pneumocytes, airspace macrophages, and interstitial inflammation.1,8,9 Rare reports of diffuse alveolar damage and acute fibrinous pneumonitis are associated with worse outcome and death.9
Despite increasing recognition that ICI pneumonitis can present unpredictably in temporality and chest radiography, focal and unilateral disease has rarely been reported. To our knowledge, only 2 prior reports have demonstrated ICI pneumonitis with pulmonary infiltrates limited to a singular lobe on chest CT, and one of these cases had an organizing pneumonia pattern on pathology as in our case.3,4 A retrospective review of ICI pneumonitis found that patients with non-lung cancer more commonly had symmetric opacities on chest CT, while lung cancer patients more commonly had asymmetric opacities.10 The authors posited that patients with non-lung cancers have a more uniform pneumonitis response as they do not have the heterogenous lung damage seen in lung cancer patients who smoked.10 However, our case of a non-lung cancer patient who was a mild, remote smoker shows that asymmetric, unilateral disease can, in fact, occur in patients without known pre-existing lung damage. Given our patient’s presentation followed a reasonable temporal sequence after pembrolizumab initiation, matched a recognized response to pembrolizumab, improved with pembrolizumab withdrawal, could not be reasonably explained by another etiology, and had previously recognized histopathology results, our patient had a Naranjo adverse drug reaction probability score of 7 consistent with probable but not definite ICI pneumonitis.11
In conclusion, ICI pneumonitis presenting with unilateral disease can be quite severe and include hydropneumothorax. Given the high potential morbidity of untreated ICI pneumonitis, unusual radiographic features of ICI pneumonitis should be considered when assessing patients on immune checkpoint inhibitor therapy with focal pulmonary infiltrates.
Disclosures & Conflicts of Interest
Drs. Sanchez and Minerowicz declare no conflicts of interest. Dr. Kahn has equity in TEO Science, FVC Health, Quantum Labs, and CoapTech, and he has received consulting fees from Chronius and Biohaven. Dr. Kluger has received institutional research grants from Merck, Bristol-Myers Squibb, and Apexigen. Additionally, Dr. Kluger has received personal fees from Iovance, Immunocore, Celldex, Merck, Elevate Bio, Instil Bio, Bristol-Myers Squibb, Clinigen, Shionogi, Chemocentryx, Calithera, Signatero, Gigagen, and GI Reviewers.
Funding Information
None.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgement
None.
Corresponding author
Andrew Sanchez, MD
Yale University Department of Internal Medicine
333 Cedar Street, P.O. Box 208056
New Haven, CT, USA 06510
Phone: 203.688.9503
Email: andrew.sanchez@yale.edu