Background
Allopurinol, a commonly prescribed medication for gout helps reduce uric acid serum levels by inhibiting the enzyme xanthine oxidase. Oxypurinol is the active metabolite of allopurinol and is responsible for most side effects. Allopurinol can cause rare and severe adverse reactions including Stevens-Johnson syndrome. Bone marrow toxicity is an extremely rare but serious side effect of allopurinol. We present a patient with severe neutropenia and aseptic meningitis related to allopurinol without the presence of HLA-B*5801 allele.
Case Presentation
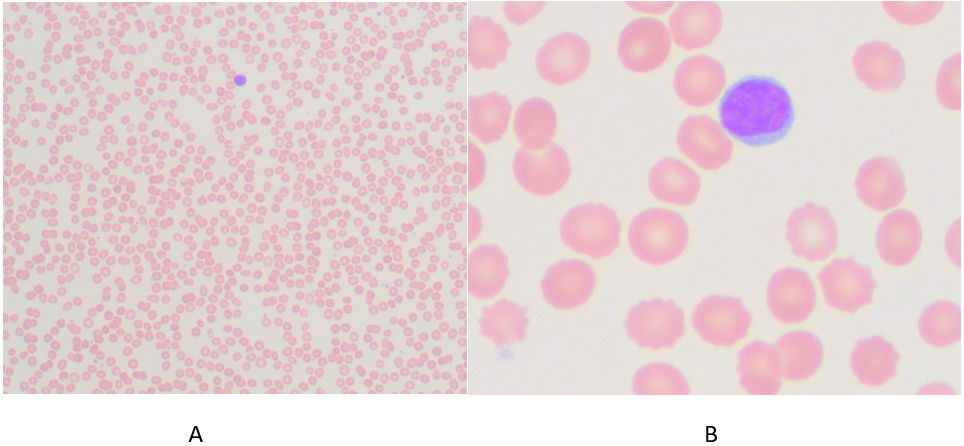
A 68-year-old man arrived at the emergency room after being found delirious at home. On initial evaluation, he was noted to be confused, with tachycardia and hypotension. Workup showed severe leukopenia with absolute neutrophil count (ANC) of 0.09 x109/L, hyponatremia, acute renal failure (ARF), lactic acidosis, and elevated creatinine kinase (Table 1). Further workup showed mildly decreased hemoglobin, normal platelet count, vitamin B1, and vitamin B12. Urine osmolality and urine sodium levels were suggestive of hypovolemic hyponatremia. Computed tomography (CT) of the head showed a left posterior scalp hematoma related to a laceration from a fall, and an MRI brain showed no acute intracranial abnormality. CSF analysis showed significantly increased protein, glucose, red blood cells, and lymphocytes with negative culture results. Cryptococcal antigen was negative. Serum blood cultures resulted positive for Staphylococcus epidermidis. He was managed in the intensive care unit with aggressive hydration, broad-spectrum antibiotics, and vasopressor support. The source of bacteremia was suspected to be from cellulitis in his right arm, and with aggressive supportive treatment, he showed clinical improvement with a resolution of delirium. Despite the clinical recovery, his white blood cell (WBC) count continued to be low, with an ANC of 0.09 x109/L on day 2. His peripheral blood smear review showed a significant decrease in neutrophils, normochromic red cells, burr cells, and morphologically normal platelets (Figure 1).

Upon thorough questioning, the patient mentioned a previous hospitalization six months prior with a similar presentation. At that time, he was treated for sepsis and severe neutropenia and underwent bone marrow aspiration and biopsy revealing a normocellular marrow with trilineage hematopoiesis. At that time, he had taken allopurinol 300 milligrams daily for gout for approximately two months and had stopped the medication after discharge. The patient resumed allopurinol approximately three weeks prior to this presentation. On hospital day two, allopurinol was stopped, and on day four WBC count started improving to 6 x 109/L and normal ANC on Day 5 (Table 1). A bone marrow biopsy was not repeated since the neutrophil count improved with allopurinol discontinuation. Other laboratory tests also showed improvement in renal function, creatinine kinase, and serum lactic acid. Testing for HLA-B*5801 allele was negative.
Discussion
Agranulocytosis is defined by a neutrophil count less than 0.5 x109/L. Advanced age is one of the major risk factors for drug related agranulocytosis.1,2 The International Agranulocytosis and Aplastic Anemia Study (IAAAS) defined drug induced agranulocytosis as neutrophil counts less than 0.5 x109/L and neutrophil counts less than 0.1 x109/L with fever or other signs of infection. Since there may be multiple factors leading to agranulocytosis, the following findings make the index of suspicion high for a particular drug to be the etiology: onset of agranulocytosis within seven days of initiation of the drug or during treatment, neutrophil count increasing to 1.5 x109/L within a month of discontinuation of the drug, recurrence of agranulocytosis upon reintroduction of the drug and exclusion of other causes of neutropenia including but not limited to congenital causes, chemotherapy, recent infections.3 The true incidence of drug-induced agranulocytosis is unknown. Medications with higher risk of this adverse effect are clozapine, sulfasalazine, anti-thyroid medications and penicillamine.4 Presentation can be varied depending on the drug, but septic shock-like presentations have been reported. The mechanism of agranulocytosis is largely immune mediated such as immune-mediated destruction of neutrophils, antibody production mediated by the drug and direct toxic effects on granulocyte precursors.5,6
Allopurinol is a relatively safe and effective uric acid lowering treatment for gout. Drug reaction with eosinophilia and systemic symptoms syndrome (DRESS), hepatotoxicity and dermatological reactions have been reported with allopurinol. Hematological side effects are rare but aplastic anemia has been reported.7 Serious side effects like hypersensitivity are rare and may have a high morbidity and mortality (around 9-20%).8 Allopurinol hypersensitivity is primarily mediated by an oxypurinol-specific T cell response.9 One other case of allopurinol-induced agranulocytosis has been reported. The bone marrow aspirate in that case was hypocellular without any neutrophils, their precursors and without nucleated red cells. In contrast, our patient had normal bone marrow appearance with severe peripheral neutropenia.10
The risk factors for allopurinol hypersensitivity include concomitant diuretic use, renal impairment, and genetic factors like HLA-B*5801 allele, which is more common in individuals of Asian descent.11 The risk of developing severe allopurinol hypersensitivity in those with HLA-B*5801 and renal impairment is estimated to be 18%.12 Our case has pathognomonic features of drug induced agranulocytosis. Given that prior discontinuation of allopurinol led to normalization of his cell counts and new symptoms began after self-reintroduction makes it likely that this presentation was drug-induced. Agranulocytosis has been attributed to multiple medications, and a comprehensive review of patient’s medications should be a priority in patients with a low neutrophil count. Table 2 lists the most common non-chemotherapeutic drugs with agranulocytosis. Our patients’ Naranjo drug reaction probability score was 6, which is a “Probable” (score 5-8) cause for the adverse reaction. Cessation of allopurinol led to significant improvement in symptoms and laboratory parameters. The treatment of drug-induced agranulocytosis is mainly supportive, including discontinuation of the offending agent.13 Granulocyte colony-stimulating factor (G-CSF) can be considered to improve neutrophil counts.14
In conclusion, physicians must be aware of drug-induced agranulocytosis, especially when other more common causes are eliminated. The presence of HLA-B*5801 allele is a known risk factor for severe allopurinol hypersensitivity in certain patient populations, and future research may be aimed at identifying other risk factors for hypersensitivity in individuals without this allele.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding Statement
No funding was obtained for this manuscript.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
None.
Corresponding author
Aswanth Reddy, MD
Department of Hematology and Oncology
Mercy Clinic
7001 Rogers Ave
Fort Smith, AR 72903
Emal: aswanth404@gmail.com