Background
Varicella Zoster Virus (VZV) is a neurotropic DNA alpha herpesvirus that infects more than 95% of the world’s population.1 It results in primary infection and then becomes latent in neuronal ganglia. It travels transaxially, and its manifestation pattern depends on whether it travels centripetally or centrifugally.1 VZV-associated vasculopathy is an underdiagnosed condition.1 It predicates to small vessels in 37% of cases and large vessels in 13%. The remaining 50% have involvement of both.2 Large vessel involvement is more predominant in the anterior circulation, and multifocal involvement is more common in immunocompromised individuals.3
Case Report
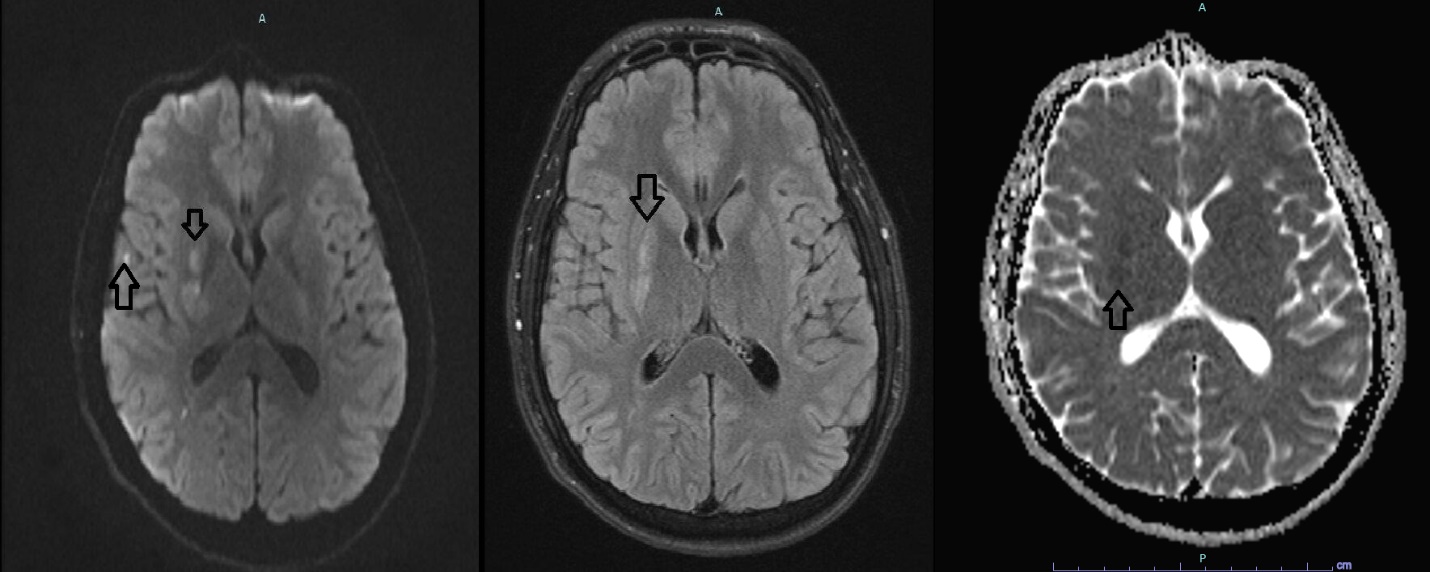
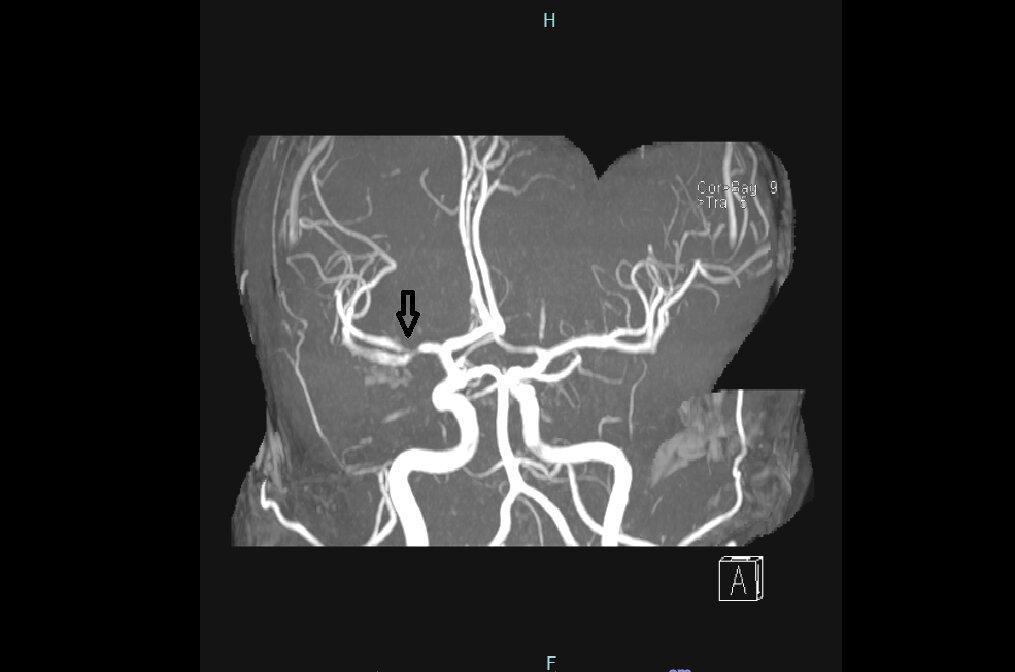
A 30-year-old male presented to the emergency department (ED) for severe bilateral and constant headache associated with left upper extremity (LUE) weakness and facial paresthesia affecting the entire right facial side. His past medical history was significant for migraine and depression. He reported that the headache quality was different from his usual migraine attacks. His home medications included only clonazepam. He was not able to recall his immunization history. There was no family history of strokes. Physical exam showed left upper extremity weakness ⅗ with diminished light touch sensation. Physical exam of the face was unremarkable for weakness nor sensory loss. No evidence of skin rash was seen. Vital signs showed a blood pressure of 125/75 mmHg and a heart rate of 64 beats per minute. Magnetic resonance imaging (MRI) showed areas of restricted diffusion on the right gangliocapsular region (Figure 1). Magnetic resonance angiography (MRA) showed severe focal stenosis of right distal M1 and proximal M2 without extracranial stenosis (Figure 2). Transthoracic echocardiography (TTE) was unremarkable. However, transesophageal echocardiography (TEE) showed patent foramen ovale with evidence of bidirectional shunt by agitated saline study. Extensive workup for hereditary thrombophilia and systemic vasculitis was unyielding. Dual antiplatelet therapy was started along with statin, and he was discharged.
_mri_on_the_left_showing_areas_of_restricted_diffusion_in_periventric.jpeg)
.jpeg)
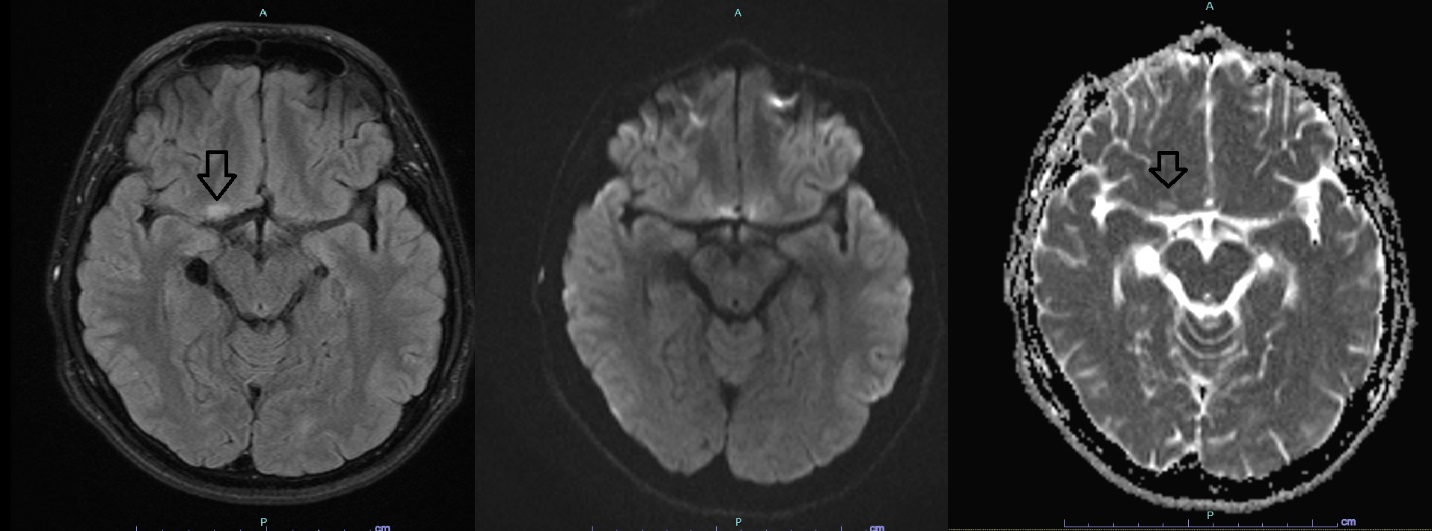
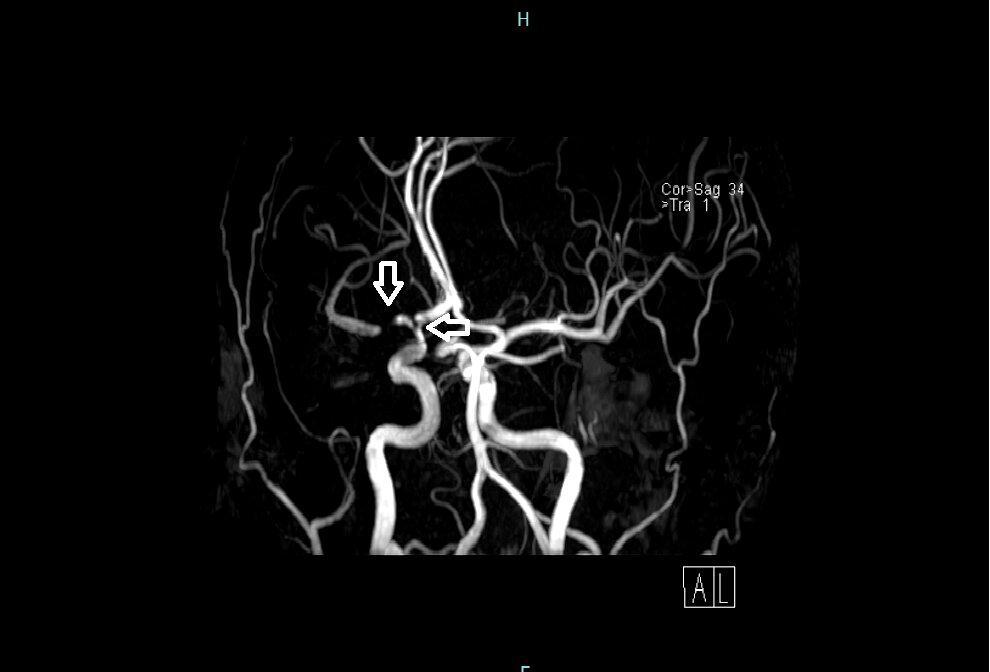
One and a half months later, he followed up with his outpatient neurologist for a worsening headache. A follow-up MRI and MRA were obtained. MRI of the brain showed a small new focus of hyperintensity in fluid-attenuated inversion recovery (FLAIR) in the right frontal lobe without corresponding restricted diffusion (Figure 3). MRA showed progression of previous findings with new moderate stenosis of the right distal internal carotid artery and severe stenosis at the origin of M1 and A1 (Figure 4). Clinically, his weakness and numbness had improved. Physical exam was unremarkable, including an intact touch sensation and 5/5 muscle power on the LUE. Basic labs were unremarkable. Diagnostic cerebral angiography showed the same findings with mild focal stenosis of the right posterior communicating artery origin and significant collaterals to middle cerebral artery (MCA) distribution from other major arteries.
_.jpeg)

The patient lacks risk factors of atherosclerosis including hypertension, diabetes and hyperlipidemia. Hemoglobin A1c was normal at 4.7%. Lipid panel showed total cholesterol at 138 mg/dl, HDL at 69 mg/dl and LDL at 61 mg/dl. There was a strong suspicion of cerebral vasculitis. Thus, a lumbar picture (LP) was pursued. Cerebrospinal fluid (CSF) analysis showed lymphocytic pleocytosis with white blood cell count (WBC) of 20 cells/ml (reference range less than 5 cells/ml), elevated protein of 67 mg/dl (reference range 12-60 mg/dl) and normal glucose of 55 mg/dl (reference range 40-60 mg/dl). CSF culture was unyielding. An extensive workup for systemic vasculitis was unremarkable. However, varicella zoster virus (VZV) polymerase chain reaction (PCR) was positive with elevated VZV IgG titer at 3.864 (more than 165 is considered positive) but negative IgM (less than 0.90). Otherwise, meningitis/encephalitis panel was unyielding. Human immunodeficiency virus (HIV) and Rapid Plasma Reagin (RPR) were negative. He denied any history of chickenpox or recent exposure. He also denied any history of a recent rash. He was started on intravenous acyclovir. After two weeks, neurological deficits showed moderate clinical improvement. Two months later, he showed significant clinical improvement at a follow up appointment.
Discussion
VZV-associated vasculopathy can be seen during both primary infection and reactivation in immunocompetent and immunocompromised individuals and can be unifocal or multifocal. It can affect small or large arteries or, most often, a combination of both. It mainly affects the brain and spinal cord with various manifestations, including ischemic strokes, hemorrhagic strokes, subarachnoid hemorrhage, cerebellitis, cranial nerve palsies, cerebral venous sinus thrombosis, retinal necrosis, vascular stenosis, dissection, and aneurysm formation. These can present as motor or sensory deficits, but also monocular visual loss, temporal artery infection mimicking giant cell arteritis, or prolonged headache are possible. Lack of rash does not preclude the diagnosis and is found only in two-thirds of cases. Although no data are available in adults, VZV-associated strokes in children are preceded by a history of chickenpox, only in 44% of cases.1 Cerebrospinal fluid analysis usually reveals lymphocytic pleocytosis in ⅔ of cases. A normal analysis does not rule out VZV infection.4 Pleocytosis can also be seen without CNS infection.5 The usual treatment is intravenous acyclovir for 7-14 days which is used in preference to oral preparation given lower CNS bioavailability.6 The use of steroids is controversial and may be harmful.4
In this case, atherosclerosis was unlikely stroke mechanism given lack of risk factors, lack of calcification and lack of evidence of atherosclerosis elsewhere. Despite having a patent foramen ovale, the diagnosis of embolic stroke was considered unlikely given the lack of clinical and ultrasound evidence of thrombosis and unyielding workup for hereditary thrombophilia. Despite the suggestive location of intracranial stenosis, Moyamoya angiopathy was also considered unlikely given the lack of angiographic evidence of collateral meshwork of overgrown and dilated small arteries (moyamoya vessels) as well as other features like aneurysms and unilateral presentation. Systemic vasculitis was also ruled out by an extensive workup. Although nonspecific, involvement of M1 of MCA and distal ICA is common in VZV-associated vasculopathy and should raise suspicion of the diagnosis. Therefore, our leading diagnosis was VZV-associated vasculopathy, confirmed by PCR.
VZV is unique because it is the only proven virus to replicate within arteries and induce vasculopathy. However, HIV and CMV have also been suggested to induce vasculopathy but have not been pathologically confirmed. Pathological evidence suggests vascular remodeling and granulomatous arteritis, ranging from necrosis to demyelination. The risk of stroke in those with herpes zoster increased 2–9% in the first year after infection, with a higher risk in people under 40 years old, regardless of the immunological status.7 It was recently reported to be associated with deficiency of cytosolic DNA sensor RNA polymerase 3 which might explain its occurrence in immunocompetent individuals.8
Diagnosis is usually confirmed by CSF analysis for VZV DNA and Anti-VZV IgG. Anti-VZV IgM antibodies can also be detected in serum or CSF, but the lack of which does not rule out the diagnosis.9 VZV DNA has a sensitivity of 30%, while the Anti-VZV IgG antibody has a sensitivity of 93%. Therefore, a negative VZV DNA does not preclude the diagnosis. VZV DNA is usually reactive in the first seven days of symptoms onset and remains reactive for 50 days. Anti-VZV IgG antibody appears after the first seven days.10 Serological sensitivity is not different among immunocompetent and immunocompromised patients. If both are negative, the diagnosis can be reliably excluded.1 Cerebral angiogram may show areas of stenosis, but negative tests should not rule out the diagnosis as it may affect only small vessels. CSF analysis is usually significant for lymphocytic pleocytosis with elevated RBC count and protein concentration. Cerebral angiography is also helpful to demonstrate stenoses but cannot rule out the diagnosis if negative as it may be a small vessel predominant disease.2
This case serves to remind clinicians that VZV vasculopathy should always be suspected in young patients with stroke, evolving stroke, multifocal stroke, primarily if affecting gray-white matter junction, multifocal intracranial stenosis, especially stenosis of M1 of MCA and the terminal portion of ICA. In this case, initial impressions and investigations were directed to systemic vasculitides and moyamoya angiopathy. However, an unyielding investigation prompted consideration of CSF analysis and investigation for VZV reactivity. This case also highlights that lack of history of chickenpox or recent zoster should not drive the investigations away from VZV. The diagnosis of this treatable cause of stroke is often missed because one-third of patients have no history of zoster rash, one-third of patients have normal CSF, and there is an average 4.2-month delay from zoster to neurological symptoms and signs, with VZV DNA often absent in CSF.11
DISCLOSURES/CONFLICTS OF INTEREST
The authors of this paper have no disclosures.
AUTHOR CONTRIBUTION
All Authors (MAA, HA, MK) have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
- Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
- Drafting the work or revising it critically for important intellectual content; AND
- Final approval of the version to be published; AND
- Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding Author
Mohammad Abu-Abaa, MD
Capital Health Regional Medical Center
Internal Medicine Residency Program
750 Brunswick Ave, Trenton, NJ
Mabu-abaa@capitalhealth.org
Phone 609 635 8152
ORCID ID 0000-0003-1752-1235