A 51-year-old woman with a medical history of acute rheumatic fever during her childhood presented with non-productive cough, dyspnea at rest, orthopnea, and paroxysmal nocturnal dyspnea. She was diagnosed with rheumatic heart disease and mitral valve stenosis eight years before her current presentation. Her comorbidities are atrial fibrillation, congestive heart failure and systemic hypertension. Her home medications were digoxin 0.25 mcg, carvedilol 12.5 mg, warfarin 5 mg, spironolactone 50 mg, furosemide 40 mg, and sacubitril/valsartan 50 mg twice a day.
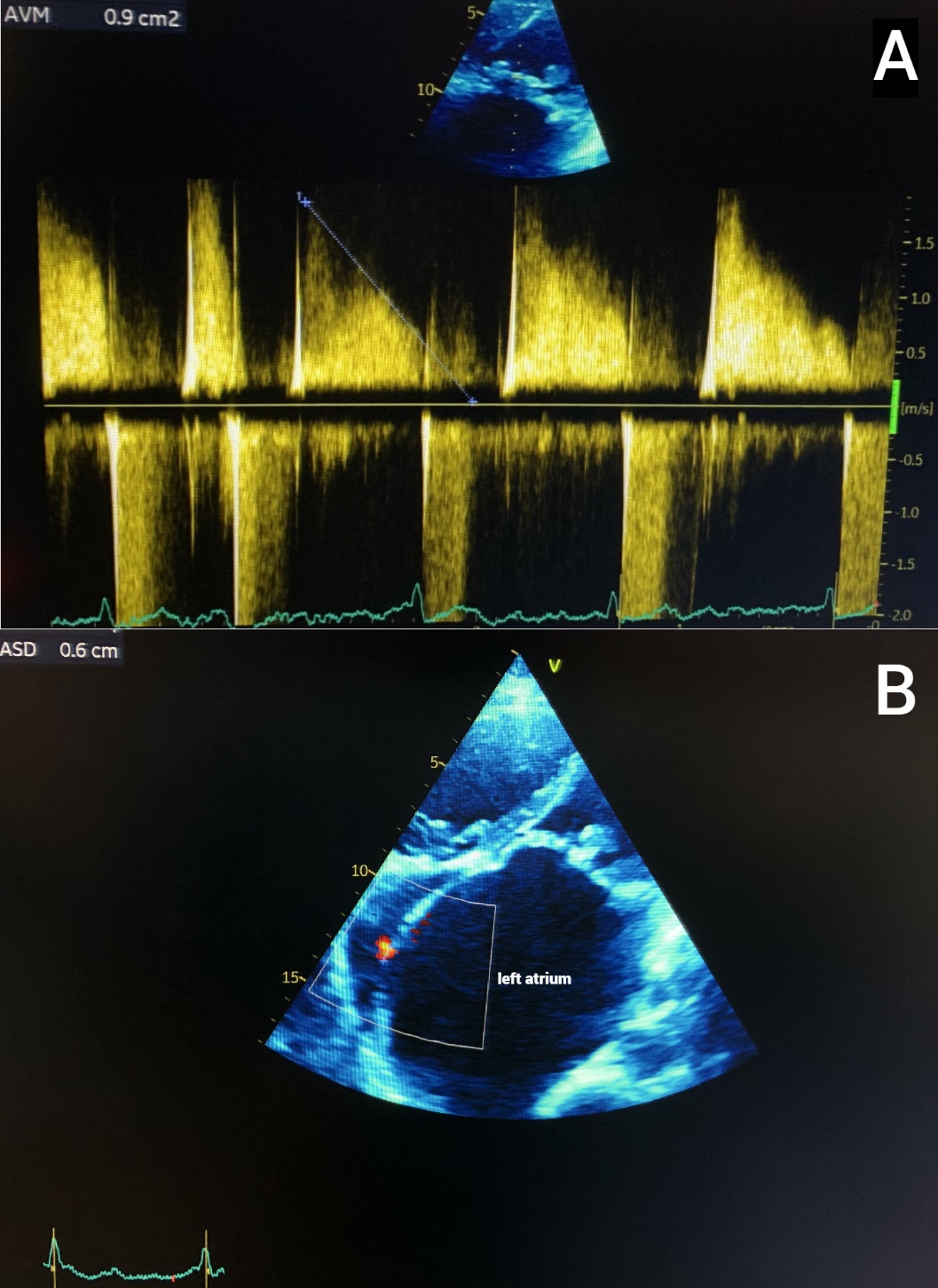
On physical examination, she was tachycardic (102 beats per minute), and tachypneic (36 breaths per minute). The exam was notable for jugular venous distension and irregularly irregular heart rhythm. She also had a grade II holosystolic murmur at the mitral area that radiated to the axilla, along with accentuation of the pulmonic component of the second heart sound and diastolic rumbling. She also had hepatomegaly and positive hepatojugular reflux. Electrocardiography revealed atrial fibrillation with rapid ventricular response and a right bundle branch block. A Chest X-ray showed cardiomegaly, bi-atrial enlargement, and pulmonary congestion. On echocardiography, she had severe mitral stenosis (mitral valve area of 0.9 cm2, peak gradient of 12.28 mmHg) and moderate mitral valve regurgitation (effective regurgitant orifice of 6.5 cm2) along with an atrial septal defect with left to right shunt and severe pulmonary hypertension (70 mmHg) (Figure 1). She was admitted to the hospital for an exacerbation of her heart failure and mitral valve replacement. Unfortunately, she died in the postoperative period because of her advanced heart failure.

Lutembacher’s syndrome (LS) was first described in 1916 and is defined as any combination of atrial septal defect (ASD) (congenital or iatrogenic) and mitral valve stenosis (congenital or acquired).1 The incidence of patients with mitral stenosis and ASD is 0.6-0.7%. Its predilection is female sex because ASD and rheumatic mitral stenosis are more prevalent in females.2 It has been reported that 40% of the patients have a medical history of rheumatic fever.3 In its pathophysiology, there is a left-to-right shunt through the ASD. The flow direction depends on the compliance of the ventricles. The right ventricle adapts easier to volume overload in normal conditions, but after chronic exposure, it enlarges and produces the clinical spectrum of right heart failure.4 The mitral stenosis and consequent dilation of the left atrium predisposes the patient to arrhythmias such as atrial fibrillation, which can be the form of presentation of this syndrome.3
They can also present with signs and symptoms of right heart failure because of pulmonary hypertension, such as jugular engorgement, systolic murmur in the pulmonic valve area, and systolic murmur in the tricuspid valve area.3,5 Patients will ultimately develop Eisenmenger syndrome (ES) because of increased pulmonary vascular resistance. The initial left-to-right shunt will become a right-to-left shunt, resulting in significant hypoxemia and cyanosis, and worsening their prognosis.6
The gold standard to diagnose LS is by echocardiography. It also helps to determine the severity of the disease. It is classified as mild mitral valve stenosis when the mitral valve area (MVA) is greater than 1.5 cm2, mean gradient (MG) lower than 5 mmHg and pulmonary arterial pressure (PAP) lower than 30 mmHg; moderate mitral valve stenosis if the MVA is between 1.0 – 1.5 cm2, MG between 5-10 mmHg and PAP between 30-50 mmHg; and severe mitral valve stenosis if the MVA is lower than 1.0 cm2, MG greater than 10 mmHg and PAP greater than 50 mmHg.3
This pathology traditionally has been treated with open surgery, but the defects can be repaired percutaneously with transcatheter closure of the ASD and balloon valvuloplasty of the mitral valve.7 Percutaneous therapy can be conducted if the ASD pulmonary-systemic (Qp/Qs) ratio is above 1.5, moderate to severe MS with symptoms with a valve morphology favorable for the procedure, pulmonary hypertension except patients with ES. Contraindications include the presence of a left atrium thrombi, absence of adequate rims around the septal defect, anomalous pulmonary drainage, grade 3 mitral regurgitation, bicommissural calcification and lack of expertise.2 If surgery is not an option, the symptoms of heart failure can be improved with guideline-directed medical therapy.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
AUTHOR CONTRIBUTION
All Authors (VAGL, AFMC, NGAB) have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
CORRESPONDING AUTHOR
Vilma Alejandra Gomez Lara, MD
Department of Internal Medicine
Clinica Murillo Hospital
Barrio Los Andes, 10th-11th ave, 8-9 st NW
21101 San Pedro Sula, Cortes, Honduras
Email: vagomez@unah.hn