Background
Nonbacterial thrombotic endocarditis (NBTE) was originally described by Ziegler in 1888 when vegetative thrombi were described on normal or degenerated cardiac valves associated with chronic inflammatory states.1 The condition has since been clarified in literature to represent the deposition of thrombi composed of platelets with strands of fibrin on heart valves with a predilection towards the aortic and mitral valves without evidence of active bacteremia.
Case Presentation
A 64-year-old man with a past medical history of remote intravenous drug use (IVDU) and a new presumptive diagnosis of metastatic lung cancer presented to his primary care physician for work up of suspected malignant lesions in the axial skeleton and persistent shortness of breath. One week prior, the patient presented to an outside hospital with complaints of three months of dyspnea and low back pain. Chest radiographs revealed left hilar prominence with a streaky opacity in the left upper lung zone. Subsequent thoracic and lumbar spinal MRI revealed spinal metastases with a pathological compression fracture of the T11 vertebral body. He was presumptively diagnosed with metastatic lung cancer and advised to follow up for tissue biopsy and further coordination of oncologic care.
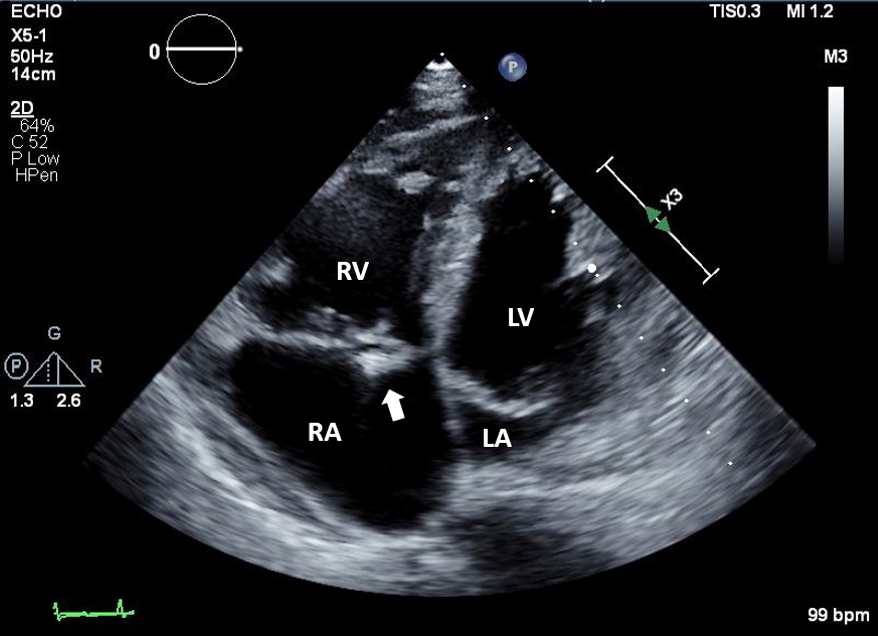
During the follow-up visit, he was noted to be tachypneic, tachycardic, and hypotensive and was referred to the hospital emergency department (ED) for stabilization and likely inpatient admission. Vital signs at arrival to the ED demonstrated a heart rate of 115 beats per minute, blood pressure of 97/69 mmHg, respiratory rate of 18 breaths/minute, and oxygen saturation of 100% on room air. Physical examination was notable for the patient being unable to complete a sentence without visible dyspnea, a III/VI systolic cardiac murmur at the left lower sternal border, and decreased breath sounds over his posterior left middle and lower lung fields. There was no evidence of Janeway lesions (non-tender erythematous macules or papules found on palmar soles and toes), Osler’s nodes (tender pink, purple nodules), or splinter hemorrhages. Laboratory studies were remarkable for neutrophilic leukocytosis and mild hypercalcemia. Computed tomography with angiography of the chest demonstrated a 3.0 cm lesion in the left apex, invasive mediastinal mass/adenopathy, large pericardial effusion, and no evidence of pulmonary embolism. A transthoracic echocardiogram (TTE) exhibited a small pericardial effusion, and a 0.8 cm mobile echo-bright density was seen on the right atrial side of the tricuspid valve concerning for vegetation (Figure 1).

Three sets of blood cultures were drawn. The patient was subsequently admitted to the general medical ward with infectious disease, hematology and oncology, cardiology, and palliative care consultations. An extensive investigation for etiologies for infective endocarditis was performed: including serologies for Q fever, Bartonella henselae, Bartonella quintana, Brucella spp, Salmonella spp., and Rickettsia spp. Blood culture specimens were held for 21 days for fastidious organisms. All serologic tests and blood cultures were negative and did not identify an infectious etiology. A simultaneous inpatient workup for his malignancy was pursued. Supraclavicular lymph node biopsy was performed with pathology demonstrating metastatic non-small cell carcinoma that was epidermal growth factor receptor and B-Raf mutation negative, without evidence of differentiation of adenocarcinoma or squamous cell carcinoma.
The patient’s history of IVDU was of concern as an etiology for the bloodstream and cardiac infection. However, the patient had been in substance use sobriety programs and denied active use for eleven years. Once infective endocarditis was adequately ruled out, the consensus among the treating physicians was that the tricuspid valve vegetation represented NBTE. The patient was started on subcutaneous enoxaparin 1.5 mg/kg every 24 hours as indicated for the treatment of thromboembolism in a patient with active malignancy. By hospital day eleven, the patient’s condition had stabilized. After goals of care discussions, he was enrolled in hospice to focus on comfort care and died within 30 days of discharge from the acute medical ward.
Discussion
Patients who develop NBTE tend to be hypercoagulable secondary to underlying autoimmune diseases or malignancy, with the most common cancers associated with NBTE being lung, pancreatic, and gastric. The majority of patients who develop NBTE remain asymptomatic until embolization occurs, which is only noted in about 42% of the patients.1 Clinical manifestations result from embolization rather than valvular dysfunction. While there are no pathognomonic symptoms or signs associated with NBTE, there are situations where NBTE should be considered: a new cardiac murmur in the setting of malignancy, lab evidence of disseminated intravascular coagulation (DIC) or signs of embolization to the central nervous system or coronary arteries.2
NBTE requires high clinical suspicion and warrants that infective endocarditis be excluded. Prior to the diagnosis of NBTE, infective endocarditis, including Coxiella spp, Bartonella spp, Brucella spp, Listeria monocytogenes, and HACEK organisms (Haemophilus sp, Actinobacilius actinomycetemcomitans, Cardiobacterium hominis, Eikenella rodens and Kingella sp), must be considered and appropriately ruled out.3 Despite a reported incidence of approximately 0.9% in the adult population, the diagnosis of NBTE is most commonly made at the time of autopsy.4
It is hypothesized that immune complexes damage the endothelium leading to the deposition of platelets and fibrin into the subendothelial connective tissue. Patients with severe pulmonary disease, including pulmonary malignancy, may have higher levels of circulating tissue factor secondary to the hypoxic environment, leading to hypercoagulability.5 While lesions are most commonly detected with echocardiography, a definitive diagnosis of the disease requires tissue biopsy of the valvular vegetation. This invasive procedure may not be tolerated well, especially in hypercoagulable states, and is commonly deferred in this patient population, as the risk of the procedure may outweigh the benefits. Cardiac magnetic resonance imaging does not have a clear role currently.5
Treatment of NBTE is aimed at treating the underlying disease while providing anticoagulation to prevent propagation of vegetations and further thromboembolic events. Current treatment suggested by guidelines are unfractionated heparin or low molecular weight heparin at therapeutic doses for thromboembolism.6 Direct oral anticoagulants have gained greater ground for their use in prophylaxis against thromboembolic disease in patients with active malignancy, however, their use in patients with NBTE has not been well-described.7 One report identified a patient who had mitral and aortic vegetations develop while on rivaroxaban for the treatment of pulmonary embolism. After transitioning to unfractionated heparin, the vegetations decreased on the mitral valve with no change to the aortic valve.8 Surgical intervention may be considered in settings similar to infective endocarditis; these include 1) severe, acute regurgitation, 2) obstruction causing refractory pulmonary edema, 3) cardiogenic shock, 4) failure of therapy, 5) large vegetations over 1.5 cm in size or 6) recurrent embolic episodes. However, given comorbidities and the high mortality risk in this patient population, special consideration should be given to selecting optimal surgical candidates.9 Outcomes for malignancy-associated NBTE are poor, given the association with advanced and often incurable cancer. Treatment options with palliative benefit, including antitumor and anticoagulant therapy, should be considered for patients with NBTE.2
The valvular lesions of NBTE most commonly affect the aortic and mitral valves, although all valves can be affected. Vegetations are often seen on the atrial surfaces of the mitral and tricuspid valves and the ventricular surfaces of the aortic and pulmonic valves.1,2 In this case, the vegetation was seen on the right atrial surface of the tricuspid valve. While right-sided valvular lesions are the least common, the reported number of tricuspid and pulmonic valve cases varies in the literature. In one autopsy series of 99 cases of NBTE, tricuspid valve involvement was seen in 9% of patients, and pulmonic valve involvement was seen in 2%. At the same time, other reports indicate lower incidences for both.1,10 Additionally, three reports of isolated tricuspid valve NBTE have been described.
This case of tricuspid valve NBTE represents the high clinical suspicion needed for identifying this rare disease process. The patient’s active pulmonary malignancy, in addition to the thorough work-up and exclusion of infective endocarditis, led the medical team to the diagnosis of NBTE. While NBTE is more commonly found on the mitral and aortic valves, this case is notable for tricuspid involvement. We theorize that the patient’s prior history of IVDU may have made his tricuspid valve more susceptible to endothelial injury in the setting of his hypercoagulable state.
DISCLOSURES/CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose.
AUTHOR CONTRIBUTION
All Authors (AMG, EEC, CXH, ADY) have reviewed the final manuscript prior to submission.
All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
- Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
- Drafting the work or revising it critically for important intellectual content; AND
- Final approval of the version to be published; AND
- Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Corresponding Author
Emily E. Cantor, MD
Hospitalist, VA Greater Los Angeles Healthcare System
Associate Clinical Professor, University of California Los Angeles David Geffen School of Medicine
11301 Wilshire Blvd, Building 500, Room 3248, Los Angeles, CA 90073
(310) 478 – 3711 extension 42473
Email: emily.cantor@va.gov