Background
Extra-respiratory manifestations, such as gastrointestinal (GI) symptoms are not uncommon among patients with COVID-19.1 Intussusception is a rare cause of bowel obstruction in adults, accounting only for 1-5% of bowel obstruction adult cases.2 While bowel obstruction has not been the mainstay of the GI COVID-19 manifestations, 25 pediatric cases, and three adult cases of intussusception have been reported so far.3–25 This case report aims to draw attention to the development of intussusception as a possible result of COVID-19 infection in the adult population and therefore guide less invasive management in these patients.
Case report
A 37-year-old woman with no significant past medical history, presented to hospital with one day of abdominal pain, nausea, and vomiting. She described the abdominal pain as severe and localized at the right lower quadrant (RLQ). She additionally reported nausea and multiple emesis episodes with inability to tolerate any oral intake. She did not report any diarrhea or hematochezia. Three days prior to the onset of her gastrointestinal symptoms, the patient, who was unvaccinated against COVID-19, developed lower back pain, chills, and myalgias. Household members were symptomatic and positive for COVID-19; therefore, she underwent a test herself that was also positive.
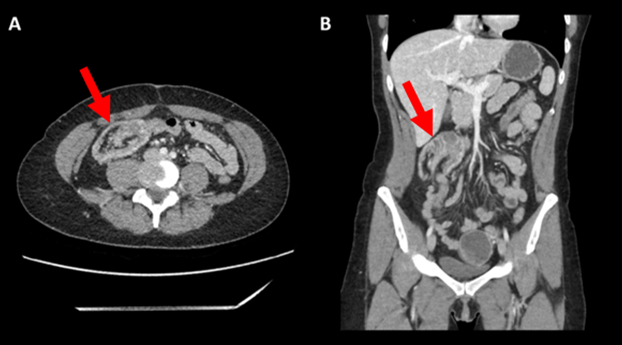
She presented to the hospital afebrile and hemodynamically stable. On exam, she had mild tenderness at the RLQ on deep palpation without guarding or rebound tenderness. She had unremarkable initial laboratory analysis with her white blood count being 4.04 K/uL, creatinine of 0.78 mg/dL, and liver function tests (LFTs) within normal limits. A computed tomography (CT) of the abdomen and pelvis with intravenous contrast demonstrated ileocolonic intussusception, without evidence of mechanical obstruction with some thickening of the small bowel within the large bowel, which was presumed to represent hypertrophied lymph nodes or a lead point mass (Figure 1). A CT of the chest revealed a patchy airspace consolidation within the right lower lung lobe consistent with pneumonia. She was started on ampicillin-sulbactam to cover for possible aspiration pneumonia.
_and_coronal_(b)_views_of_ct_abdomen_pelvis_at_the_intussusception_level__ileocol.png)
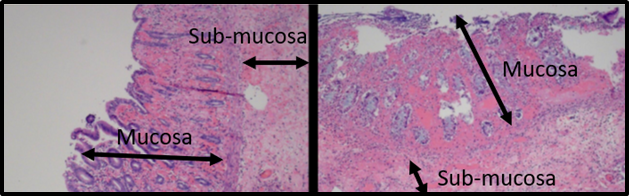
Given the abdominal findings, the patient was taken to the operating room (OR) on the same day. Intraoperatively, a clear ileocolonic intussusception was identified, without visible evidence of bowel ischemia and no suggestion of mass lesion. However, due to concern for potential malignancy causing the intussusception, a laparoscopic right hemicolectomy with ileocolic anastomosis was performed without any complication. Pathology showed mucosal necrosis and ulceration with an ischemic pattern of injury, associated with an acute inflammatory infiltrate, as well as submucosal edema, findings consistent with intussusception (Figure 2). Immunohistochemical stains for cytomegalovirus and herpes simplex virus were negative.

She was treated with remdesivir for COVID-19 pneumonia. On post operative day 5, she developed new onset lower abdominal pain with nausea and one episode of emesis. A repeat CT abdomen/pelvis with intravenous and oral contrast revealed diffuse small bowel dilation, favored to reflect ileus, without evidence of abscess or bowel perforation. The ileus resolved within one day with bowel rest. The patient did not develop any further symptoms and was discharged one week after her surgery.
Discussion
Given that the majority of adult intussusception cases are related to a lead point that pertains an increased risk for malignancy, management of adult intussusception is in most cases surgical resection.2 Our case report suggests that COVID-19 may be implicated in the development of intussusception.
This is the fourth overall case report of adult intussusception and the second ileocolonic intussusception that could potentially be attributed to COVID-19 infection. In our patient, intussusception was the initial and only clinically apparent manifestation of the disease. The patient presented with GI symptoms secondary to small bowel obstruction (SBO) as a result of ileocolonic intussusception. She did not develop any respiratory symptoms during her hospitalization. No mass was identified intraoperatively. The patient was additionally tested for human immunodeficiency virus (HIV), as acquired immunodeficiency syndrome (AIDS) -related lymphoid hyperplasia has previously been implicated in idiopathic intussusception adult cases. The patient was negative for HIV.
A comparison of our case with the other documented cases of adult intussusception that could potentially be linked to COVID-19 is presented in Table 1. The patient described here had similar CT abdomen findings to the patient described by Jackson et al., that also presented with ileocolonic intussusception. The pathology report in Jackson et al. and Gargouri et al. are also consistent with ours, showing ischemic necrosis and inflammation of the bowel.23,24 Unlike the other three case reports, our patient never had leukocytosis throughout her hospitalization except for a mild elevation on post-operative day one that resolved within 24 hours, most likely related to the surgical insult. Finally, while in the Gargouri et al. case the cecal cystic duplication is a congenital abnormality that could potentially make this patient more prone to intussusception, our patient did not have any such predisposing factors.24
Thus far, in the literature there is one additional case report of a COVID-19 positive adult that developed intussusception, which however was not attributed by the authors to the infection per se. This was a 70-year-old female that was initially hospitalized with COVID-19 pneumonia and subsequently developed acute necrotic pancreatitis, in the setting of a pre-existing large umbilical hernia with engagement of the stomach, duodenum, and head of the pancreas. Later in her hospital course the patient developed a jejuno-gastric intussusception in the absence of prior surgery, which is the single most important risk factor for that particular intussusception type. The authors did not feel that this could be directly related to COVID-19 infection, but rather to the organ herniation as described above that increased intra-abdominal pressure secondary to cough, and the presence of abdominal effusion.26
The exact mechanism leading to invagination of one portion of the bowel into an immediately adjacent one in the setting of COVID-19 infection is not fully understood yet, but this presentation could possibly be related to bowel peristalsis changes as a result of viral replication in the intestinal cells. Lymphoid hypertrophy of the intestinal Peyer’s patches could also be contributing to this presentation. While in pediatric intussusception the most prevalent etiologic factor is viral infections, in adults 65% of the cases are associated with malignancy.3,27 Hence, the management of choice in the vast majority of adult intussusception cases is surgical resection, while surgical or endoscopic reduction is avoided to eliminate the possibility of peritoneal carcinomatous seeding.2,28
As the awareness regarding COVID-19-mediated GI manifestations increases COVID-19 may be more frequently considered in the differential diagnosis of non-mass related intussusception in adult patients.29 This consideration could subsequently guide further decisions regarding less invasive management in this patient population, including surgical / laparoscopic reduction without colectomy, or even endoscopic reduction.28,30–32 Given the absence of malignancy in such cases, and provided that there is no necrotic tissue in the setting of early diagnosis, avoiding unnecessary bowel resection and its potential side effects would be of utmost importance for the recovery of these patients.
DISCLOSURES/CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose.
AUTHOR CONTRIBUTION
All Authors (MA, AMB) have reviewed the final manuscript prior to submission.
All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Corresponding author
Ana Maria Bensaci, MD
Division of Infectious Diseases, Mass General Brigham, Salem Hospital, Salem, MA, USA
81 Highland Avenue, Salem, 01970, MA, USA
9783544009
ABENSACI@PARTNERS.ORG
ORCID ID: 0000-0003-1703-7531