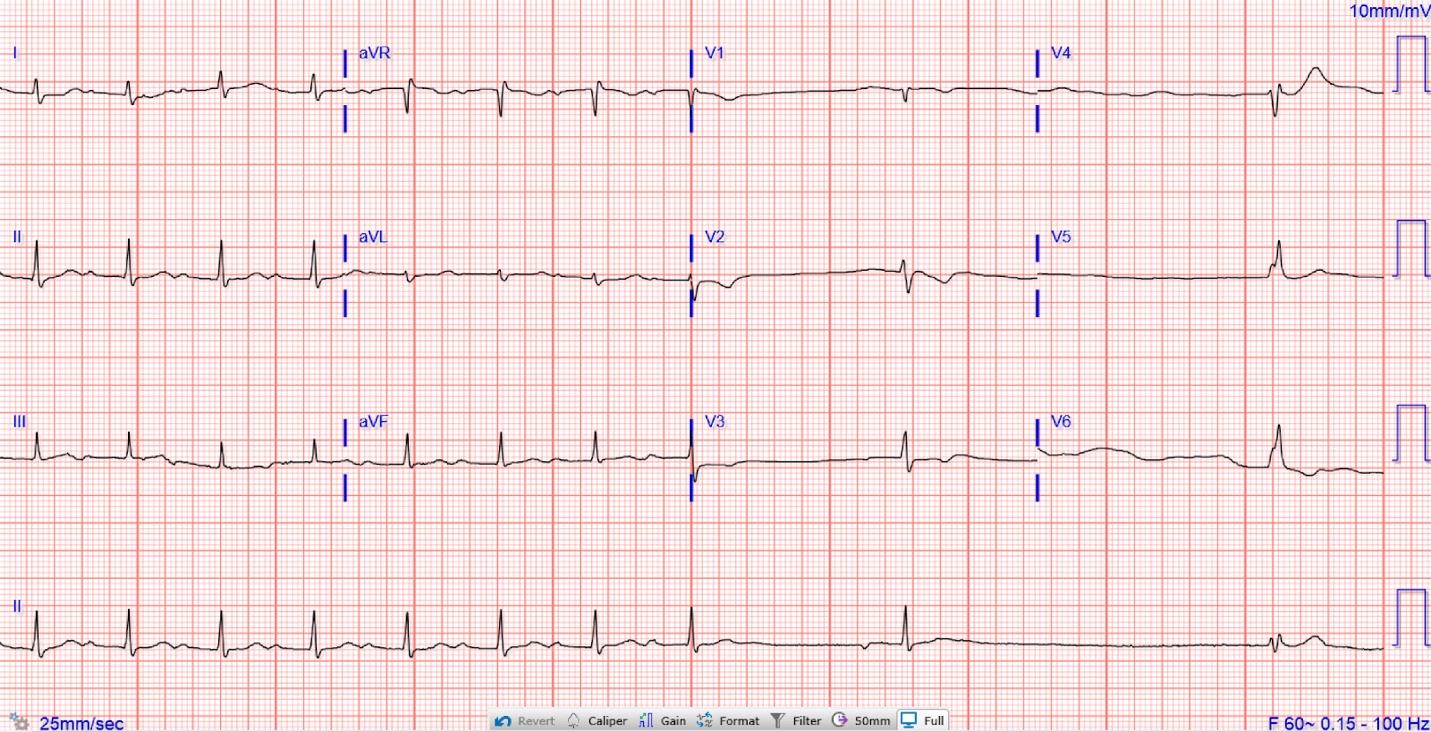

A 34-year-old female living in the Northeastern United States with no significant medical history presented to the hospital with three weeks of dry cough, dizziness, shortness of breath, headache, and chest pressure. She was in her usual state of health until she started developing a dry cough after cleaning a parrot cage at the pet store where she worked. Two weeks later, she developed dizziness without any prodromal symptoms. The dizziness occurred randomly, would last several seconds, and resolved without intervention. About one week later, she developed substernal chest pressure with exertion and occasional palpitations. She eventually presented to her primary care physician’s office with these complaints. Her primary care provider (PCP) performed an EKG, which showed a sinus pause with ventricular escape beat (Figure 1), and subsequently recommended the patient present to the emergency room.

In the hospital, she had stable vital signs with an unremarkable physical exam. Serial troponins were negative. Other labs showed WBC 7100/uL (4000-11000/ul), RBC 4.03 M/ul (4-6 M/uL), Platelets 225,000/uL (150,000-420,000/uL), Aspartate transaminase 26 U/L (10 - 35 U/L), Alanine transaminase 18 U/L (10-35 U/L), Alkaline phosphatase 99 U/L (9 - 122 U/L), Total bilirubin 0.5 mg/dL (<=1.2 mg/dL), Total protein 8.1 g/dL (6.6-8.7 g/dL), and Albumin 4.3 g/dL (3.6 - 4.9 g/dL). Chest x-ray, CT chest angiography, and bedside echocardiography were benign. While in the emergency department, she was resting in bed when she developed symptoms of near syncope. Telemetry and subsequent EKG showed various conduction patterns, including atrial flutter (Figure 2), atrial fibrillation, and complete heart block with spontaneous return to sinus rhythm. Pacer pads were placed, and she was admitted to the cardiac intensive care unit.

History obtained later in the hospital course revealed that she lives close to the woods, goes hiking often, and has been employed at the local pet store for several months. She did not recall any recent tick bites but had three ~4 cm erythematous patches on her abdomen several weeks before, for which she did seek medical attention. At the time, she was treated for ringworm infection by her PCP.
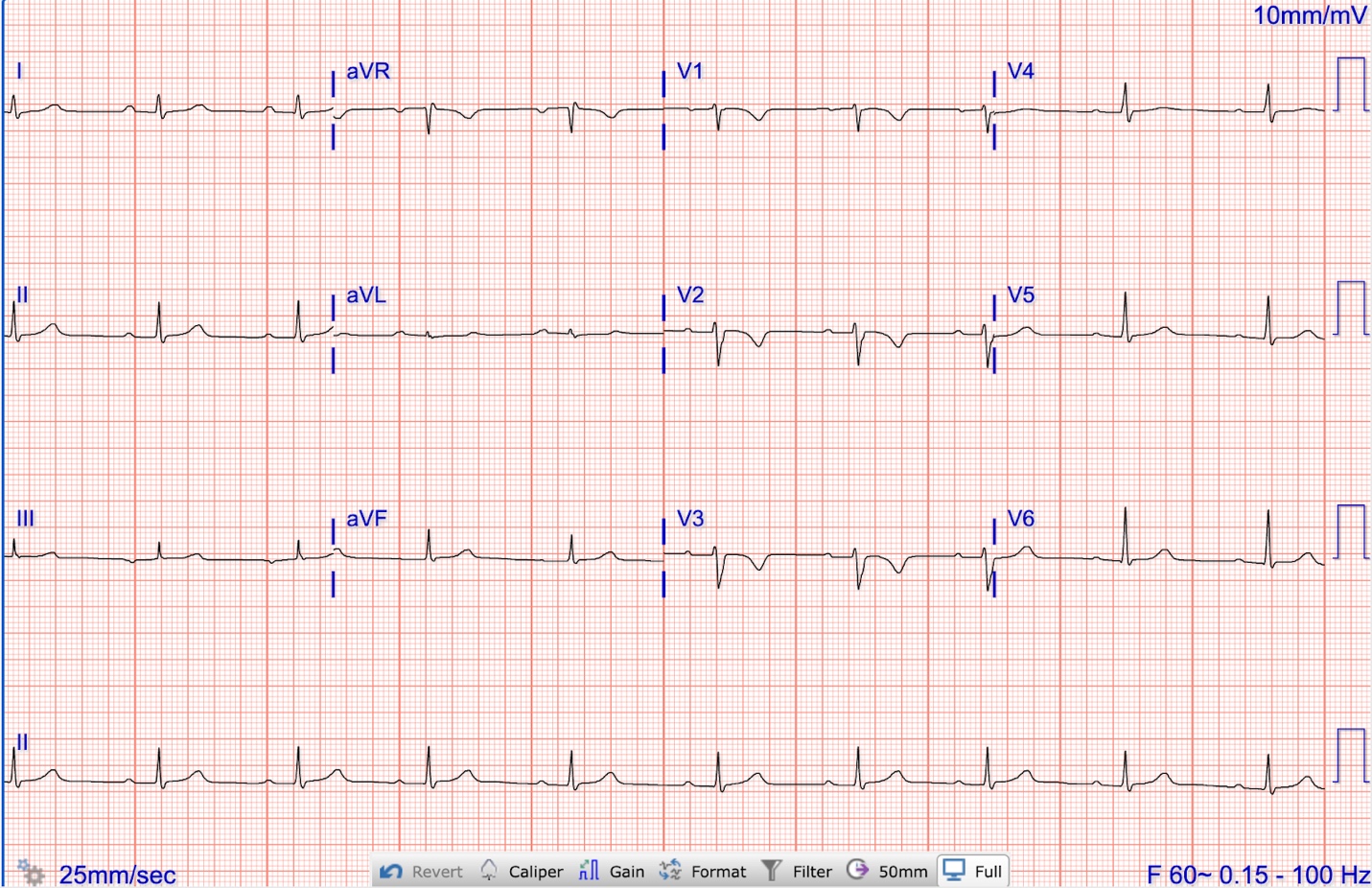
The episodic sinus pauses and the subacute onset of symptoms, in addition to her young age, negative troponins, and nonischemic EKG findings, suggested an infectious or inflammatory etiology rather than a cardiac etiology. Telemetry showed occasional sinus pauses, atrial fibrillation, and atrial flutter during admission. She was treated empirically for Lyme carditis while awaiting serology results. Within 48 hours of initiating intravenous ceftriaxone, her conduction abnormalities improved. Our patient was managed with IV ceftriaxone until her telemetry stopped showing sinus pauses for >24 hours. This occurred on hospital day seven (Figure 3) when she was discharged on oral doxycycline 100 twice daily for two more weeks. She never required temporary pacing. However, her dry cough persisted. Based on her occupational exposure to parrots, she was started on doxycycline to treat suspected psittacosis. She completed a full course of therapy for Lyme carditis and psittacosis with the resolution of her symptoms. Lyme serologies later returned positive.

This case highlights the need for high clinical suspicion and early treatment of Lyme carditis in younger individuals living in endemic areas. Lyme carditis occurs in approximately 1% of patients with Lyme disease.1 While atrioventricular blocks are the most common conduction abnormality of Lyme carditis (77-87%), it is important to consider others, such as sinus pauses, atrial fibrillation, and atrial flutter.2,3 Lyme carditis management depends on disease severity. Mild cases with only first-degree heart block can be treated with oral doxycycline 100 mg twice daily for 2-3 weeks. Severe cases other than 1st-degree heart block abnormalities are usually treated with IV ceftriaxone 2g daily for 2-3 weeks. Additionally, this case highlights an important approach to suspected psittacosis. Having a high suspicion for this rare infectious disease is important among patients with occupational exposures. In this patient, suspicion for psittacosis was high based on her exposure to bird feces and her symptoms of dry cough and headache that persisted despite the initiation of treatment for Lyme disease. The diagnosis of psittacosis was made clinically in the setting of her ongoing cough and exposure to parrots. Further, her cough resolved with treatment with doxycycline. In conclusion, we report a rare case of a patient diagnosed simultaneously with Lyme carditis and psittacosis.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Author Contribution
All Authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Corresponding author:
Jennifer Frampton
Section of Cardiology,
Department of Internal Medicine,
Yale New Haven Hospital,
New Haven, Connecticut, USA
Email: jennifer.frampton@yale.edu