
INTRODUCTION
Secondary syphilis can cause skin lesions, which are typically, discrete pink macules or papules.1 However, it could have a wide span of skin manifestations that could mimic many diseases. Malignant syphilis is a rare form of secondary syphilis that happens usually in patients with human immune deficiency virus (HIV). We describe a case of HIV-positive patient with ulceronodular lesions and systemic symptoms.
CASE PRESENTATION
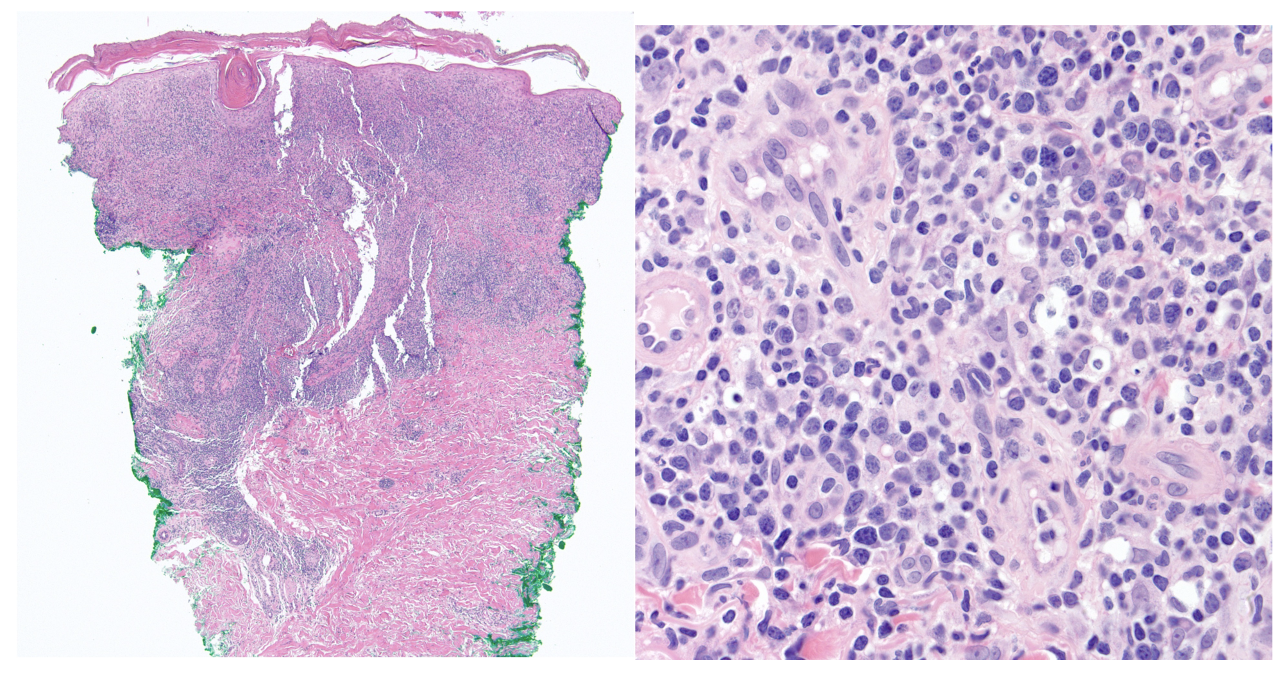
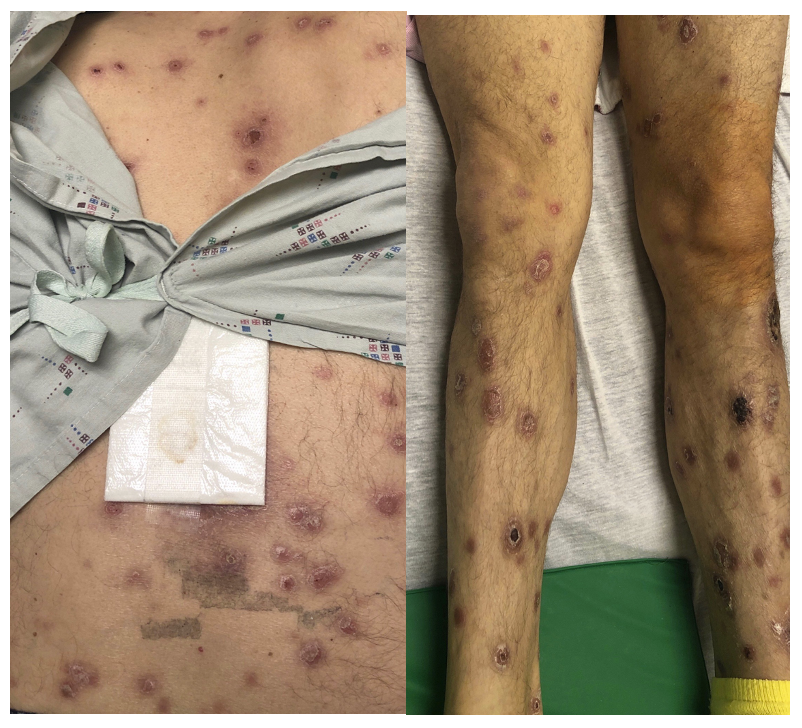
The patient is a 54-year-old male, with long standing history of HIV (CD4: 0.221 K/uL), previously treated syphilis, inflammatory bowel disease (IBD) and hypertension. He presented with a 3-week history of non-pruritic rash that spread from the face to the trunk and extremities except the palms and soles. The rash started as circular macules then became nodular; some lesions became ulcerated with subsequent crusting. Some of the lesions were foul smelling and painful. Furthermore, his dog used to lick the lesions. He has not been lately compliant with the antiretroviral regimen (bictegravir/emtricitabine/tenofovir). He complained of fever and chills a few days prior to admission. He also had fatigue throughout. He was not taking other medications and was sexually active with a female partner. He spiked fever on admission (39.4°C), otherwise the rest of the vitals were stable. The physical examination revealed skin rash without lymphadenopathy. There were well-demarcated firm pink papules and plaques with thin layer of overlying scales on the face. The rest of the skin revealed pink papules and plaques with central necrosis and scales on some lesions (Figure 1). The palms and soles were spared. Laboratory work-up showed white blood cell count of 7 x10 (3)/L (normal: 4-11 x 10 (3)/L), hemoglobin of 9.1 g/dL (normal: 13.5-17 g/dL), platelets of 335 x10 (3)/L (normal: 150-440 x 10 (3)/L), sedimentation rate of 91 mm/h (normal: 0-20 mm/hr), creatinine of 1.27 mg/dL (normal: 0.8-1.3 mg/dL), and normal liver enzymes. He was started empirically on vancomycin and ampicillin-sulbactam to treat superimposed infection. Cultures from the open painful lesions had methicillin-sensitive staphylococcus aureus (MSSA), he was treated accordingly with doxycycline. Other work-up was negative including lyme serology, thyroid function test, respiratory pathogen panel, rocky-mountain spotted fever serology, tick borne-illness serology, histoplasma urinary antigen, and serum cryptococcus antigen. Rectal gonorrhea PCR was positive, IgG was positive for HSV and VZV. HIV viral load was 35 copies/mL. Treponema palladium antibodies were positive, and RPR titers were elevated 1:32 (was previously 1:1 five years ago). The skin biopsy showed lichenoid lymphohistocytocytic and plasma cell-rich infiltrates involving the superficial dermis with deeper extension along vascular channels and adenexal structures (Figure 2). GMS, PAS-D, AFB and Fite stains were negative for microorganisms. The diagnosis of lues maligna (LM) was confirmed; the patient was treated for secondary syphilis with intramuscular benzathine penicillin G, 2.4 million units. The skin lesions eventually improved (Figure 3).


DISCUSSION
Syphilis can pose a diagnostic challenge because the skin lesions could take different forms. Malignant syphilis is a rare form of secondary syphilis, that causes specific cutaneous manifestations. The French dermatologist Pierre Bazin first coined the term malignant, and malignant syphilis was later defined by Dubue.2,3 Malignant syphilis is referred to as syphilis maligna praecox, lues maligna, ulceronodular and rupioid syphilis.2,4 LM happens more commonly in immunocompromised patients especially patients living with HIV.2 HIV increases the risk of developing LM by 60 times.5 Additionally, LM has been reported in immunocompetent patients especially malnourished, diabetic, and alcoholic patients.2,4,6,7 It also happens in pregnant women and nursing mothers.7 It typically appears as an oval, papulopustular skin lesion with well demarcated borders, sometimes covered with a lamellar crust.8
The rash in secondary syphilis is usually diffuse, symmetric macular or popular eruption that involves trunk and extremities. Skin lesions in LM usually are pleomorphic round-to-oval papules, papulopustulles or nodules with ulcerations and brown lamellar crusted lesions spread over the trunk and extremities.4 The skin lesions in our patient were nodular, ulcerated and crusted, raising concern of fungal or mycobacterial infection. The ulcerated areas raised suspicion of pyoderma gangernosum since he had IBD. Herpetic infection was on the differential diagnosis. Our patient had fever, chills, and fatigue, in accordance with the described clinical course of LM.7 Fever, weight changes and headache can precede LM by at least 4 weeks.4
The high titers of RPR and the skin biopsy confirmed the diagnosis of syphilis. Biopsy is usually recommended to rule out fungal, mycobacterial, and other non-infectious causes. The biopsy also helps to rule out cutaneous T-cell lymphoma.9 The Histopathological findings are usually nonspecific; as biopsy could reveal dense infiltrate of plasma cells, lymphocytes, and histiocytes, perivascular congestions, thrombosed vessels in the dermis with endarteritis, surface parakeratosism, prominent lichenoid infiltrate, or endothelial hyperplasia.2,4,5,10 Our patient’s biopsy showed mixed inflammatory infiltrates in keeping with secondary syphilis. RPR usually ranges between 1:16 and 1:4096 in HIV-negative patients with LM, however HIV may lead to lower titers given prozone phenomenon (inability to visualize agglutination due to overabundant antibodies interference with clumping of antibody-antigen complexes).9
Histopathology usually reveals nonspecific findings with perivascular congestion and dermal plasma cell infiltrates.4 Our patient had a similar pathology with lymphocytic infiltrates that extended to the vascular structures. The clinical and pathological correlation with serological tests helped the diagnosis. Furthermore, Fisher et al, mentioned diagnostic criteria: strongly positive RPR titer; a severe Jarisch-Herxheimer reaction (JHR); characteristic gross and microscopic morphology; and rapid resolution of the lesions with antibiotics.11
It is worth mentioning that it was suggested to screen for syphilis before starting immunosuppressives, given that immunosuppression may change the course of syphilis.12
Treatment of secondary syphilis is usually benzathine penicillin G 2.4-million-unit IM as a single dose.13 Non-pregnant patients with secondary syphilis who are allergic to penicillin can be treated with doxycycline (100 mg orally twice a day for 14 days) or tetracycline (500 mg orally 4 times daily for 14 days).13 In conclusion, Lues Maligna is a rare manifestation of a common disease. Physicians should be vigilant of this diagnosis especially among HIV patients and other types of immune suppression. High clinical suspicion is the key to diagnosis.
DISCLOSURE/CONFLICT OF INTEREST
The author has no conflict of interest to disclose
Corresponding author:
Fadi Samaan, MD, FACP, FHM
Assistant Professor of Medicine, Clinical Educator
Warren Alpert Medical School at Brown University
Division of Hospital Medicine
593 Eddy St, Providence, RI, 02903
Phone: 401-444-3985
Fax: 401-444-3986
Email address: fasamaan@yahoo.com