A 43-year-old man presented with generalized weakness and unintentional weight loss. There was no history of drug addiction, blood transfusion, recent travel, or vaccination. He had no known medical co-morbidities and was not taking any medication. Physical examination revealed a temperature of 100.4°F, pulse rate of 109/min, respiratory rate of 14/min, BP of 129/91 mmHg, and pruritic, diffuse maculopapular rash involving the palms and soles. Laboratory tests revealed a white cell count of 11,300/mm3 (4,000-11,000/mm3), hemoglobin of 11.2 g/dL (13.2 - 17.1 g/dL), serum urea and creatinine concentration of 68mg/dl (8 - 23 mg/dL) and 9.94 mg/dL (0.40 - 1.30 mg/dL), serum albumin concentration of 2 g/dL (3.6 – 4.9 g/dL), and total protein of 6.5 g/dL (6.6 - 8.7 g/dL). Urine examination showed 4+ proteinuria, hyaline, and granular casts, RBCs 3, polymorphs 10-20 per high power field, and protein/creatinine (Cr) ratio was 5.72 mg/mg Cr (reference: <0.10 mg/mg Cr).
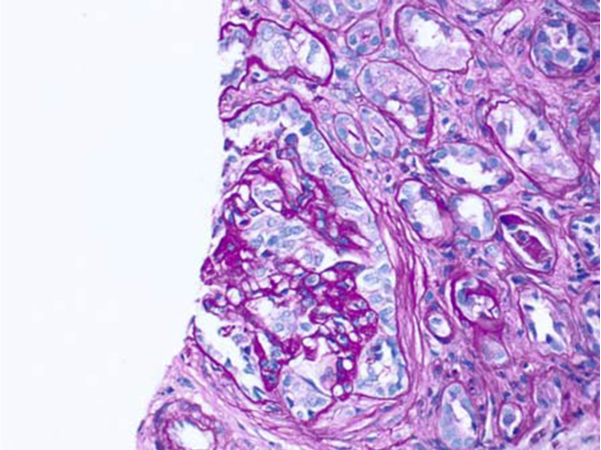
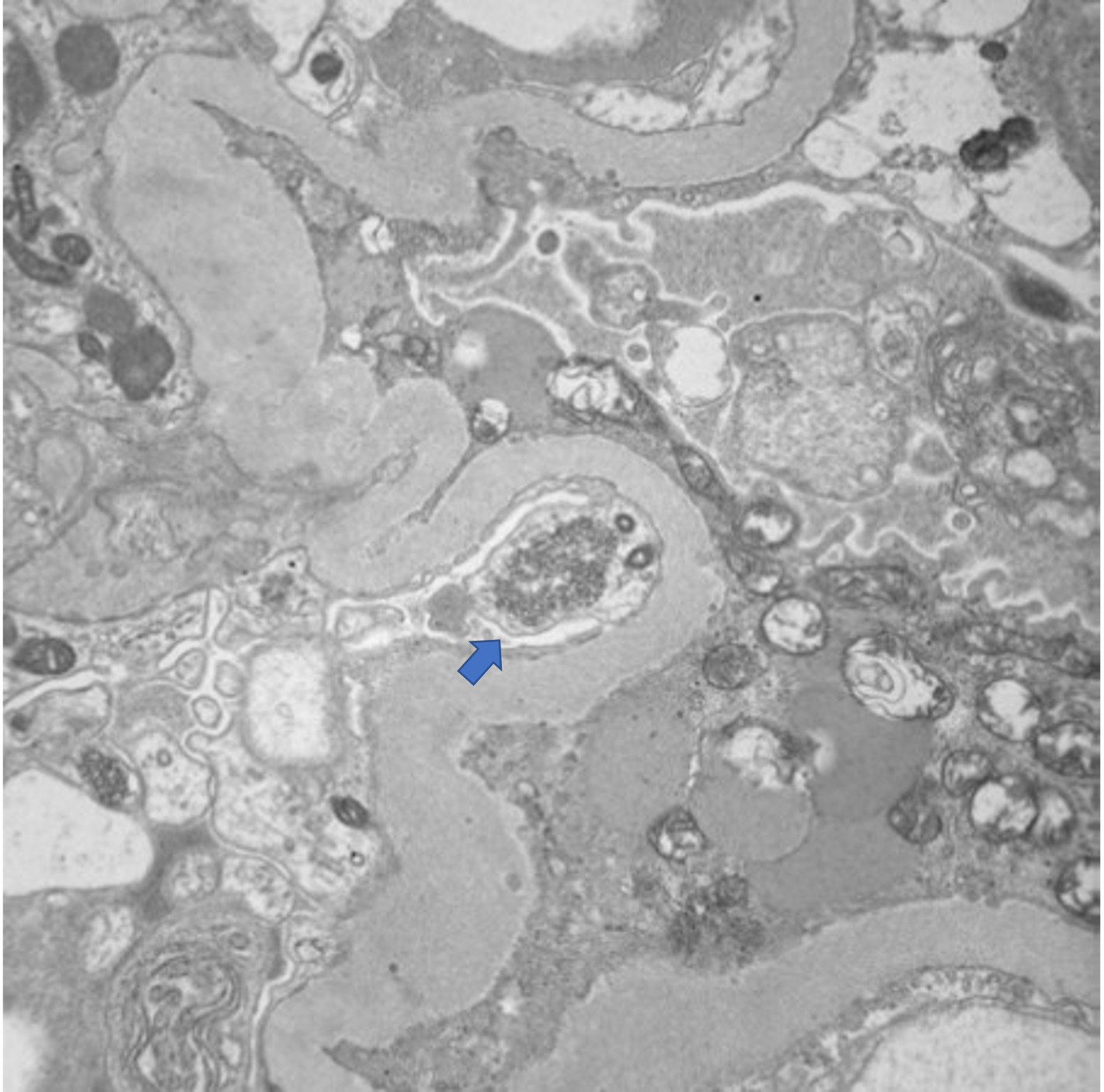
A renal ultrasound revealed normal-sized kidneys with increased renal echogenicity. His enzyme-linked immunosorbent assay (ELISA) and a Western blot assay for HIV-1 antibodies were positive. CD4 counts were 18/μL (reference: 466-1,608/μl), and HIV viral load was found to be 1,070,000/mL. Tests for HBV, HCV, and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) were negative. The patient revealed that he had unprotected sex with men months ago. Serum urea and creatinine rose and peaked at 143 and 15.3 g/dL during hospitalization. Renal biopsy showed 3 of 12 glomeruli were globally sclerotic and focal segmental glomerulonephritis (FSGS) with collapsing features (Figure 1,2). APOL1 genotyping was not performed.


He was treated with highly active antiretroviral therapy (HAART) and underwent inpatient peritoneal catheter placement with a plan to initiate outpatient dialysis. Over the months, he had significantly improved kidney function tests, with creatinine dropping to 1.9 mg/dL. However, he never started on dialysis, and the peritoneal catheter was removed four months later.
HIV-associated nephropathy (HIVAN) was first described during the HIV/AIDS pandemic in the 1980s. HIVAN typically presents as nephrotic range proteinuria, while hypertension and edema are atypical. Collapsing glomerulopathy (CG) is a classic histopathological finding of HIVAN, and tubuloreticular inclusions, characteristic of interferon-mediated viral infection, and can be found in HIVAN.1 Historically, HIVAN led to rapidly progressive ESRD; in the modern era, HAART significantly improved the prognosis of HIVAN. HAART remains the first-line therapy for HIVAN, and glucocorticoid can be used as an adjunct therapy for HIVAN on a case-by-case basis.2
HIVAN represents the severe spectrum of APOL1 nephropathy. Untreated HIV-infected patients who carry two APOL1 risk alleles have a 50% risk for developing HIVAN. APOL1 variants were hypothesized as the product of natural selection in sub-Saharan Africa to confer protection from Trypanosome brucei rhodesiense, a parasite that causes African sleeping sickness. A “second hit” such as Parvovirus B19, cytomegalovirus, and HIV-1 infection induces interferon, which increases podocyte-specific APOL1 overexpression. APOL1 causes direct cellular toxicity and death of podocytes, resulting in proteinuric kidney disease.1,2 In recent years, the attention of CS has shifted from HIVAN to COVID-19-associated nephropathy (COVAN).3 Like HIV-1, SARS-CoV-2 coronavirus induces interferon and hence COVAN shares the same collapsing features as HIVAN.1 Our case reminds us of HIVAN as a cause of CG, to allow prompt initiation of HAART.
Disclosures/Conflicts of Interest
The author has no conflicts of interest to disclose.
Corresponding author
Jia Wei Tan, MD
Department of Internal Medicine
Yale New Haven Health - Bridgeport Hospital,
Bridgeport, CT, USA
Email: jia.tan094@gmail.com