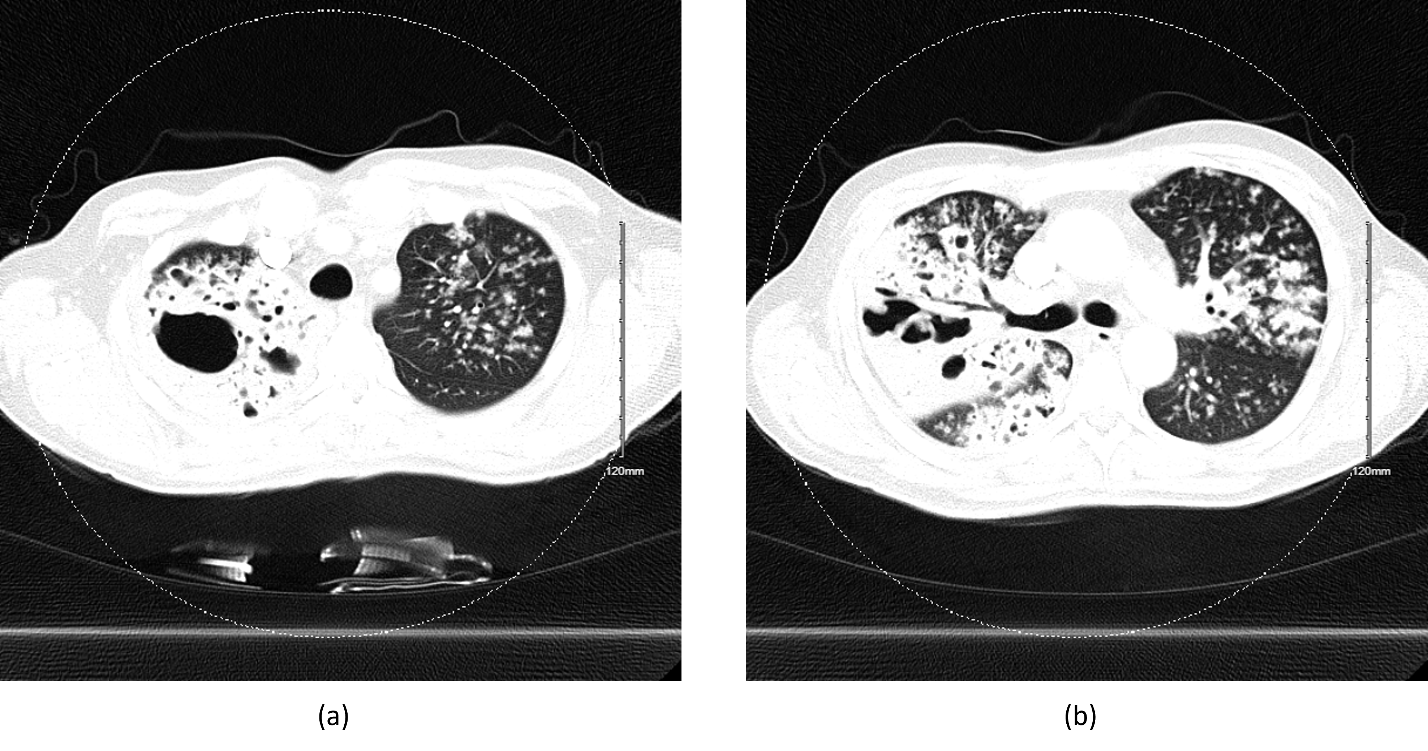
A 45-year-old Hispanic male with no history of tuberculosis (TB) or exposure presented with three months of fatigue, 25-pound unintentional weight loss, productive cough, and night sweats. He was originally from Mexico but denied recent travel, homelessness, incarceration, alcohol consumption, and smoking. COVID and HIV were negative. Computed tomography (CT) was notable for a large right upper lobe cavitary lesion (Figure 1). TB diagnosis was confirmed with positive sputum cultures for Mycobacterium tuberculosis. He was discharged on rifampin, isoniazid, pyrazinamide, and ethambutol (RIPE) under directly observed therapy (DOT) with health department follow-up and reported no side effects. The patient was compliant with TB therapy and did not miss any doses.
_ct_chest_scan_with_cavitary_lesion_in_the_right_upper_lobe_and_extensive_nodular_invol.png)
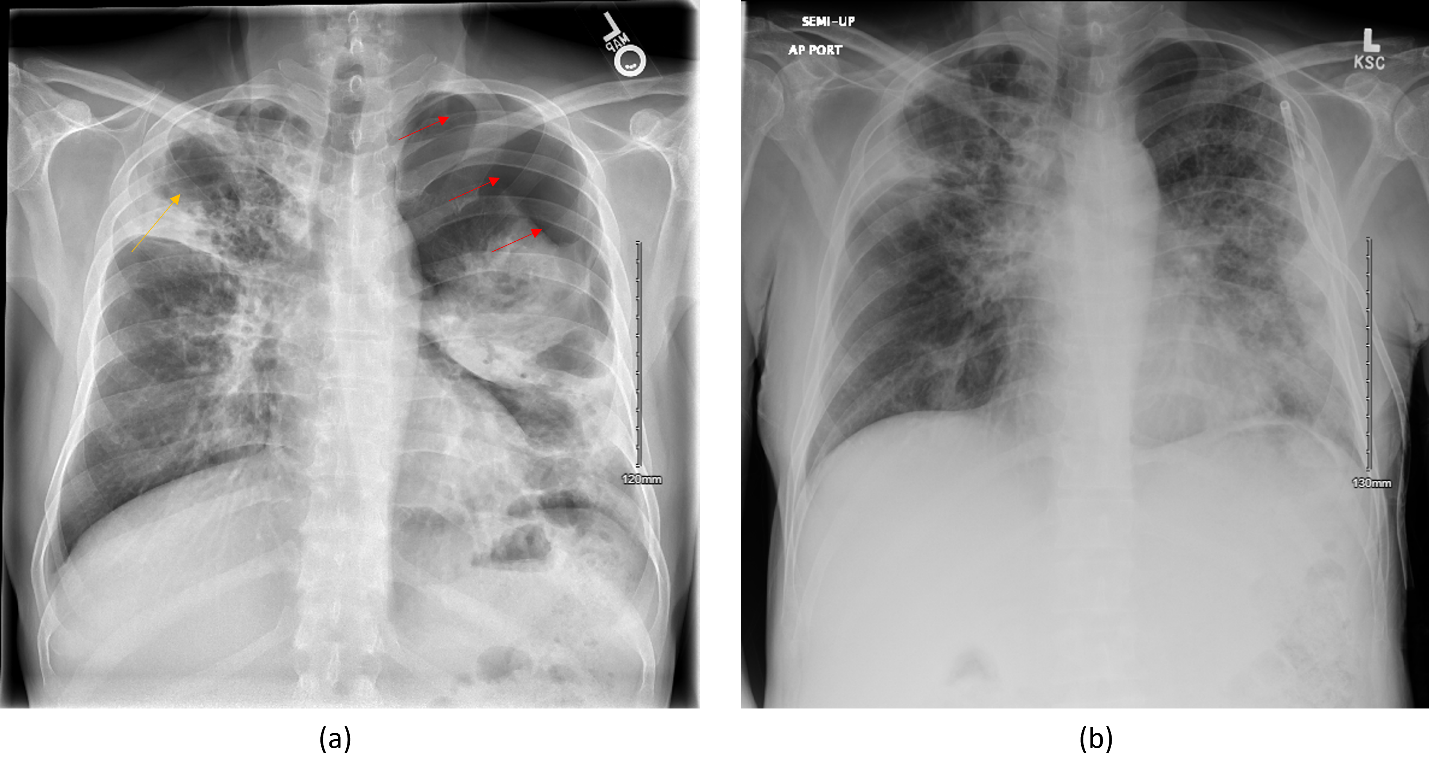
Two months after diagnosis, a routine chest x-ray (CXR) taken during DOT follow-up demonstrated a new incidental large apical left upper lobe apical pneumothorax (Figure 2a). He presented to the emergency department completely asymptomatic. His vital signs were completely normal, and he was saturating 97% on ambient air. A left chest tube was placed, resulting in significant re-expansion but residual pneumothorax. The patient was admitted for continued evaluation and management. His hospital course was uncomplicated, and daily serial CXR showed interval improvement. On admission day four, the pneumothorax resolved (Figure 2b), the chest tube was removed, and he was discharged on the previous DOT.
_two_months_after_initial_tb_diagnosis__cxr_on_admission_showing_new_left_apical_pneumo.png)
Tuberculosis (TB) is the leading infectious cause of secondary spontaneous pneumothorax (SSP), a complication that has been reported in 0.6-1.4% of TB patients.1–3 The mean age of TB-associated SSP ranges from 35-45 years, and upwards of 90% are male.4 On initial presentation, symptoms include productive cough, dyspnea, and pleuritic pain. Radiological features include parenchymal infiltration (99%), cavitation (66%), pleural thickening (25%), and fibrosis (25%).2 Chest tube placement is the first-line management in patients with large or symptomatic SSP. Surgical repair or pleurodesis may be indicated in cases complicated by persistent air leak following chest tube placement or bronchopleural fistula. Further management for SSP should be directed to the underlying etiology.
The prevalence of incidental TB-associated SSP is currently unknown due to the lack of large cohort studies. Although asymptomatic pneumothoraxes can sometimes self-resolve when small or without primary lung pathology, any large pneumothorax (>2 or 3 cm depending on the guideline) occurring in the setting of known lung disease warrants a low threshold for treatment.4–6 The proposed mechanism for pneumothorax in patients with cavitary lesions is progressive caseating necrosis and rupture of the cavity into the pleural space.7 Surprisingly, our patient’s pneumothorax occurred opposite the side of his cavitary lesion. We believe that extensive pulmonary fibrosis from TB resulted in impaired oxygen exchange, leading to an apical bleb’s development and rupture. His known cavitary lesion may become a nidus for a future right-sided pneumothorax. In summary, we present a case of a patient with recently diagnosed TB compliant on RIPE and DOT for two months who was incidentally found to have a large pneumothorax. Despite the presence of a cavitary lesion, a well-known cause for TB-associated SSP, his pneumothorax was unexpectedly found on the opposite lung field.
Acknowledgement
We thank the patient for allowing us to discuss his case and management for research purposes. We also thank the reviewers for their time and contributions to the final manuscript.
Disclosures/Conflicts of Interest
The authors declare they have no conflicts of interest.
Author Contribution
All Authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding Author
Victor Liaw, BS
5323 Harry Hines Boulevard,
Dallas, TX, USA
Telephone: 214-648-2509
Fax: 214-648-8955
Email: victor.liaw@utsouthwestern.edu