Case Presentation
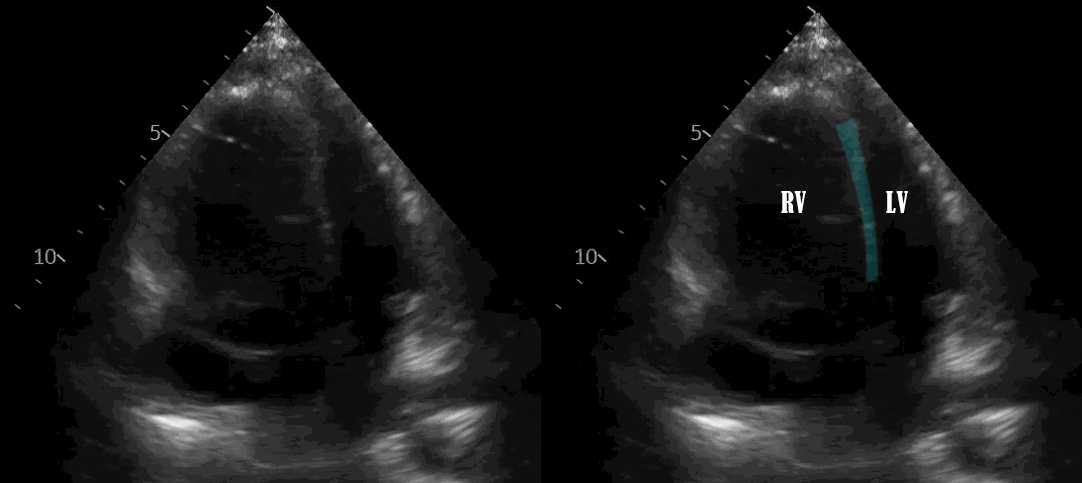
A 37-year-old female with gastroparesis and attention deficit hyperactivity disorder presented with weight loss and was admitted for severe protein-calorie malnutrition. On day 10 of admission, she had unwitnessed syncope with associated tachycardia, hypotension, and hypoxia. She received intravenous (IV) fluids without improvement and was transferred to the intensive care unit. A chest X-ray showed bilateral reticular opacities suggestive of airway inflammation. Her electrocardiogram (ECG) was notable for sinus tachycardia with diffuse non-specific ST and T-wave abnormalities. Troponin T was elevated at 0.324 ng/ml (normal <0.029 ng/mL), and NT-pro-BNP was high at 1581 pg/mL. A bedside echocardiogram showed RV systolic failure, RV dilation, and interventricular septal bowing (Figure 1). Computed tomography angiography (CTA) was negative for pulmonary embolism (PE). Right heart catheterization (RHC) revealed elevated pulmonary artery pressure, low mixed-venous oxygen saturation, and normal pulmonary capillary wedge pressure, suggestive of RV failure from acute pulmonary hypertension (PH) (Table 1). A nurse identified a foreign syringe among the patient’s belongings, and she admitted to crushing MPH pills and self-injecting into her midline catheter before her syncopal episode. Her symptoms resolved after 3 days of supportive care. A repeat echocardiogram showed normal RV size and systolic function.
_dilation_with_bowing_of_the_.jpeg)
Discussion
Methylphenidate (MPH) is a frequently abused stimulant. We present a case of transient right ventricle (RV) failure after injection of MPH. MPH is a central nervous system sympathomimetic stimulant used to treat adult narcolepsy and attention deficit hyperactivity disorder (ADHD). It is commonly abused by high school and college students, both those who have been prescribed it and those who obtain it illegally, with the majority of documented cases happening in individuals with a history of substance abuse disorder.1–4 The tablets are crushed into a fine powder for nasal inhalation or dissolved into a liquid for intravenous (IV) injection, allowing it to enter the brain quickly and produce an amphetamine-like stimulant effect characterized by brief euphoria, anxiolysis, increased focus, and intellectual capacities.1,2 This is followed by a “down” period of anxiety and dysphoria.1 Chronic IV MPH use results in significant weight loss and tolerance effect, requiring higher doses to achieve the desired euphoric effect. This eventually leads to a withdrawal syndrome characterized by abdominal pain, sweating, shivering, nausea, and vomiting.1 IV MPH has been associated with significant morbidity and mortality with several case reports describing the association with granulomatous lung disease, fatal pulmonary hypertension (PH), cerebral artery occlusion, intracranial hemorrhage, and acute hepatic necrosis.5–10
Proposed mechanisms for PH in chronic MPH use include occlusion of pulmonary arterioles by foreign body granulomas, thickening of the small pulmonary arteries and arterioles, and serotonin-mediated pulmonary vasoconstriction.8 There have been case reports describing pulmonary hypertension with chronic MPH use IV injections and inhalation.8,11 In this case, the patient admitted to crushing her MPH pills and self-injecting through her mid-line. This caused line-related upper extremity DVT, gram-positive bacteremia, and an acute rise of pulmonary artery pressure causing acute hypoxic respiratory failure and RV failure. This was evidenced by echocardiographic findings and right heart catheterization. While difficult to prove causation, the temporal relationship between self-injection and symptom onset suggests a role for MPH in this patient’s acute RV failure. Other causes for acute RV failure were ruled out: she had no prior history of PH, ECG was not consistent with ischemia, CTA was negative for PE, and RHC was not consistent with left ventricular failure. While there are case reports of persistent PH with chronic IV MPH use, this case describes the only reported incident of transient acute RV failure after IV MPH use. In conclusion, the case highlights the importance for health care providers to be familiar with the manifestations of MPH abuse.
Disclosures/Conflicts of Interest
The authors have no conflicts of interest to disclose.
Author Contribution
All Authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Arjun Chatterjee, MD
Department of Internal medicine,
Cleveland Clinic Foundation,
Cleveland, OH 44195, United States.
Telephone: 216.399.9959
Email: chattea2@ccf.org