Background
VIPoma is a rare neuroendocrine tumor that produces vasoactive intestinal polypeptide (VIP). It is most often found in middle-aged adults and toddlers. Most tumors arise in the pancreas; however, in children, they can form more often in the sympathetic chain or adrenal glands.1 We present an older adult with subacute diarrhea, hypokalemia, hypotension, and hypercalcemia who was eventually diagnosed with VIPoma.
Case Presentation
A 74-year-old woman with a history of hypothyroidism treated with levothyroxine and recent nephrolithiasis presented with fatigue, persistent subacute diarrhea, and hypokalemia. She was found to have hypotension, which resolved with intravenous (IV) fluid administration. The patient was encouraged to maintain oral intake and was given potassium supplementation.
Due to persistent symptoms over the next few months, additional work-up was completed. Infectious stool work-up was negative, but a complete metabolic panel was notable for calcium of 11.9 mg/dL (normal range 8.7-10.3 mg/dL). Her PTH was 19 pg/mL (normal range 15-65 pg/mL), 25 hydroxy vitamin D 44.1 ng/mL (normal range 30.0-100.0 ng/mL), and PTHrp <2.0 pmol/L (normal value <2.0 pmol/L). Serum protein electrophoresis and immunofixation were normal, and she did not have an M spike (Table 1). Further history revealed generalized bone pain, polydipsia, nocturia, and memory loss. In addition, she noted difficulty swallowing, prompting her to eat less, and in the setting of her ongoing chronic diarrhea, she lost 20 pounds over five months.
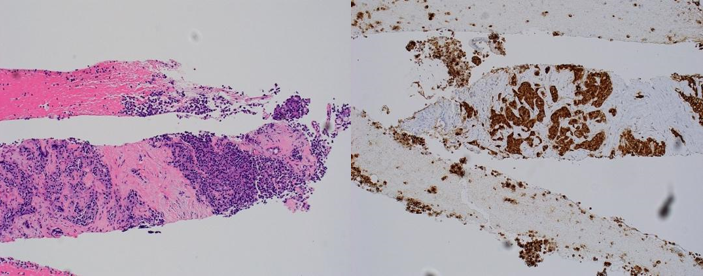
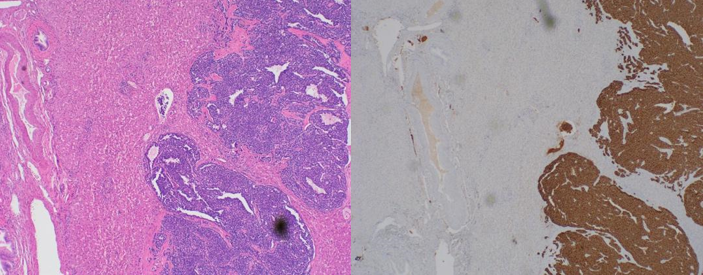
The VIP level came back high at 982 pg/mL (normal range 0-58 pg/mL) with a repeat value of 388.4 pg/mL (Table 1). A CT of the abdomen and pelvis with pancreatic protocol did not reveal pancreatic abnormalities. However, a 2-centimeter uncinate pancreatic mass was found on endoscopic ultrasound evaluation. Pathology was consistent with VIPoma (Figure 1). She was started on octreotide. A follow up CT scan of the abdomen and pelvis revealed multiple low-density lesions in the liver. She received a partial hepatectomy, and the results were consistent with metastasis (Figure 2). She received a partial hepatectomy and is planned for a Whipple procedure to remove the primary tumor.
_h_e_stain_of_endoscopic_ultrasound_fine_needle_aspiration_results_(100x)_revealing_.png)
_h_e_stain_of_the_partial_hepatectomy_(200x)_revealing_unremarkable_liver_parenchyma.png)
Discussion
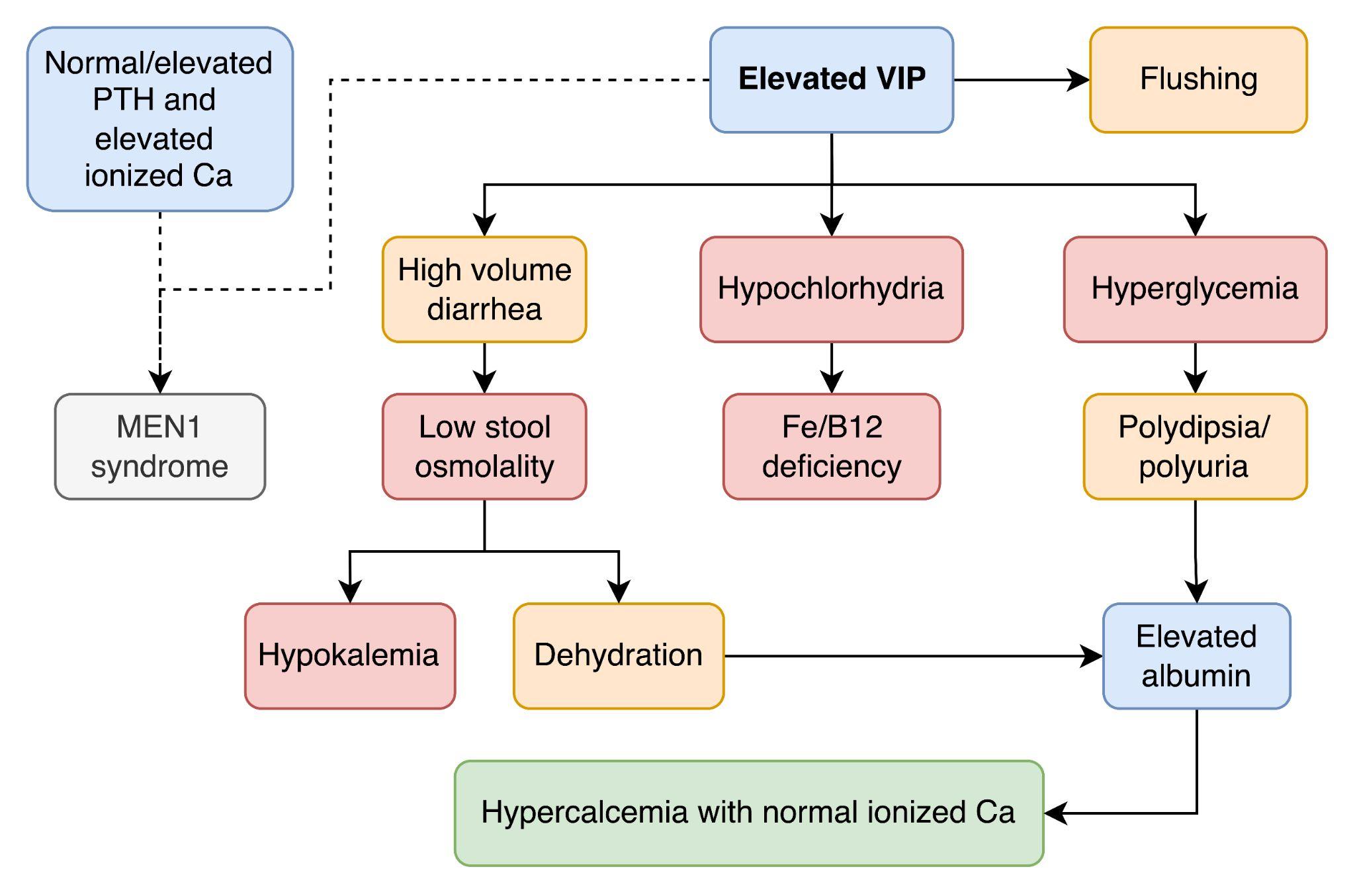
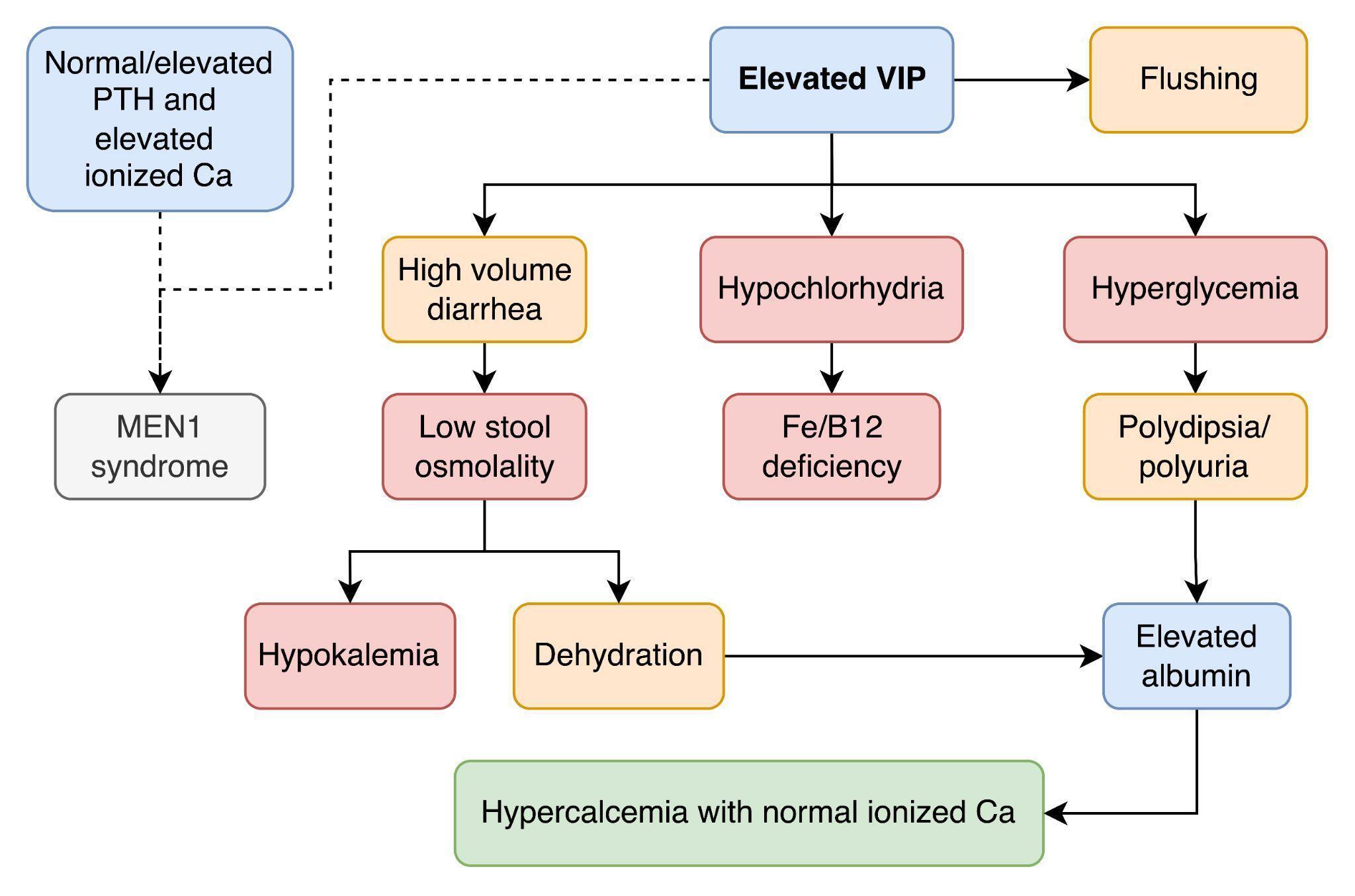
Vasoactive intestinal polypeptide acts locally on the gastrointestinal tract to induce intestinal electrolyte and water secretion. An excess of this hormone can thus cause secretory diarrhea and electrolyte abnormalities such as hypokalemia. In addition, surplus VIP can cause hypochlorhydria or achlorhydria by inhibiting the parietal cells in the stomach. This constellation of symptoms and laboratory abnormalities: Watery Diarrhea, Hypokalemia, and Achlorhydria is known as WDHA syndrome or Verner Morrison Syndrome. The inhibition of parietal cells can also cause vitamin B12 or iron deficiency. VIP secretion also causes hyperglycemia by inducing glycogenolysis and cutaneous flushing from prostaglandin release and vasoactive properties.
Another laboratory finding from having increased pancreatic secretion of VIP is hypercalcemia. Diarrhea (and to a lesser degree, polyuria from hyperglycemia) can cause severe dehydration, leading to increased serum albumin concentration and elevated serum calcium. Bone lytic lesions can lead to increased serum calcium. While most VIPomas are solitary tumors, they can be associated with multiple endocrine neoplasia 1 (MEN1) syndrome about 5% of the time.2 Family history or personal history of other MEN1 associated conditions, such as primary hyperparathyroidism or pituitary adenomas, would warrant genetic testing (Figure 3).
By the time of VIPoma diagnosis, most tumors are over 3 centimeters in size and more than 50% have metastasized.3 Diagnosis is made with two separate elevated serum VIP levels. Localization of the tumor can be made with computed tomography (CT) or magnetic resonance imaging (MRI) of the abdomen. In cases where initial imaging does not identify the tumor, endoscopic ultrasound, or positron emission tomography (PET) imaging can be utilized. Additionally, PET scans can help locate foci of metastasis.
This case illustrates the need to pursue further work-up when lab abnormalities are inconsistent with a clinical syndrome. Hypercalcemia is typically associated with constipation; therefore, the constellation of hypercalcemia and diarrhea should prompt additional investigation. While VIPoma has an incidence of one per million, it has a median survival of 96 months due to the late presentation of the disease with most cases already with metastasis.4,5 Early identification and referral to surgery is imperative for better outcomes.
Treatment of VIPoma begins with fluid and electrolyte repletion. Somatostatin analogs such as octreotide inhibit VIP release and treat symptoms such as diarrhea. However, definitive treatment occurs with resection. Staging of the disease as well as patient comorbidities would determine the approach. Common locations of metastases include the liver, kidneys, bone, and lymph nodes.2 After resection, surveillance for recurrence is performed via VIP and abdominal imaging measurements for up to 10 years.
Acknowledgement
Special thanks to the University of California Riverside/Riverside Community Hospital Internal Medicine Program Leadership as well as the American College of Physicians California Abstract and Poster Mentorship Program for their support in this case report.
Disclosures/Conflicts of Interest
The authors do not have anything to disclose.
Funding Information
No funding was required.
Author Contribution
All Authors (OPY, SC, SZ, TBM, SP) have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the ICJME criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Satya Patel, MD, FACP
David Geffen School of Medicine at University of California, Los Angeles
Greater Los Angeles Veterans Affairs Healthcare System
Mailing address: 11301 Wilshire Blvd Bld 500 Mail Code 111 Los Angeles, CA 90073
Telephone: 310-478-3711 ext 44680
E-mail: satya.patel2@va.gov