Background
Purtscher retinopathy is a chorioretinopathy associated with trauma up to 24-48 hours prior to the presentation of visual changes.1 In remote reports, the same retinal pathology with retinal hemorrhages, cotton-wool spots and retinal whitening has been associated with a non-traumatic inciting event including acute pancreatitis, renal failure, long-bone injury, chest compression, connective tissue, and hematologic disorders.2 This entity is known as Purtscher-like retinopathy and it is thought to be secondary to retinal vasculature microembolization from leukocyte aggregation resulting in arteriolar precapillary occlusion and microvascular infarct amongst the retinal layers. Microembolization can occur secondary to fat emboli, in the setting of a long bone fracture, or disseminated pancreatic proteases in the systemic circulation. Leukoembolization, complement activation with secondary lymph extravasation, acute expansion of retinal veins due to impaired venous return, and disseminated lipase after systemic injury have also been implicated in its pathophysiology.3–6 The retinal findings include the pathognomonic Purtscher flecken (areas of whitening in the inner retina between the retinal arterioles and venules), posterior pole cotton-wool spots, and retinal hemorrhages.2
We describe a case of Purtscher-like retinopathy, a rarely diagnosed complication of acute pancreatitis that has been associated with higher morbidity and mortality rates.7 Drawing attention to the importance of a thorough history and physical examination that includes assessing visual acuity and a fundoscopic exam in patients with acute pancreatitis will enhance the diagnosis rates of this pathologic entity.
Case presentation
A 33-year-old woman with past medical history of anxiety and attention deficit disorder (ADD) on amphetamine/dextroamphetamine, presented to the emergency department (ED) with abdominal pain and visual changes.
The patient reported 2 days of severe epigastric pain radiating to the back, accompanied by febrile episodes up to 102o F. She denied any episodes of diarrhea, but she did have nausea and one bilious emesis episode at the time of the pain onset. She reported profound vision changes over the same period, that started hours apart from the abdominal pain onset. She described her vision as “seeing patchy dark shadows, and areas of bright light, with objects fading” and reported inability to read, especially at a distance. The visual changes were more prominent on the left. She denied any eye pain, floaters, or flashes. The patient had no past ocular history with intact vision historically and without any previous refractive error prior to presentation.
The patient reported consuming significant amounts of alcohol that included vodka and other hard liquor daily for at least 2 weeks prior to her presentation.
The patient was afebrile, normotensive, tachycardic to 123 beats/minute, tachypneic, saturating normally on ambient air. Her abdomen was soft, non-distended, but diffusely tender, without guarding, rigidity, or rebound tenderness. Murphy’s and McBurney’s signs were negative. Her initial ophthalmologic evaluation revealed visual acuity limited to counting fingers at 3 feet distance and a fleeting glimpse of numbers on the near vision card in both eyes (OU). Her confrontation visual fields to count fingers were intact OU. Her pupils were equal and reactive to light. The anterior segment exam was unremarkable, including no signs of anterior chamber inflammation OU. Fundoscopic exam showed diffuse bilateral flame hemorrhages and retinal whitening.
Her initial blood tests were notable for leukocytosis without band forms (WBC 15.51 K/ μL; normal value 4.5-11 k/ μL), a mild elevation of the alanine aminotransferase (ALT), ALT 83 U/L (normal value 4-36 U/L), and the aspartate aminotransferase (AST), AST 43 U/L (normal value 8-33 U/L), direct bilirubin 0.5 mg/dL (normal value < 0.3 mg/dL), total bilirubin 1.2 mg/dL (normal value < 1.2 mg/dL), ESR 21 mm/h (normal value < 15 mm/h), CRP 215.7 mg/L (normal value < 0.9 mg/dL), lipase of 256 U/L (normal value < 160 U/L), triglycerides of 73 mg/dL (normal value < 150 mg/dL), and calcium of 9.5 mg/dL (normal value 8.5-10.2 mg/dL). Toxicology studies were positive for amphetamines in the urine (attributed to amphetamine/dextroamphetamine intake for ADD management). Ethanol levels were undetectable.
Microbiology was notable for negative COVID-19 nasopharyngeal testing. Blood cultures were negative. A hepatitis panel as well as human immunodeficiency virus were also tested and were both found to be negative.
Computed tomography (CT) of the abdomen and pelvis showed acute necrotizing pancreatitis with heterogeneous enhancement of the pancreatic head and uncinate process, a likely developing acute necrotic collection in the left upper quadrant adjacent to the inferior tip of the liver, peripancreatic stranding, phlegmonous change, and small volume abdominopelvic ascites. She underwent CT brain angiography without evidence of any intracranial or cervical arterial stenosis, occlusion, aneurysm, or vascular dissection.
The patient was admitted to hospital for management of acute necrotizing pancreatitis with intravenous hydration and pain management with clinical improvement. Repeat CT of her abdomen and pelvis confirmed pancreatitis improvement. An ophthalmology evaluation was performed in the hospital and no acute treatment of the retinal pathology was recommended while in the hospital.
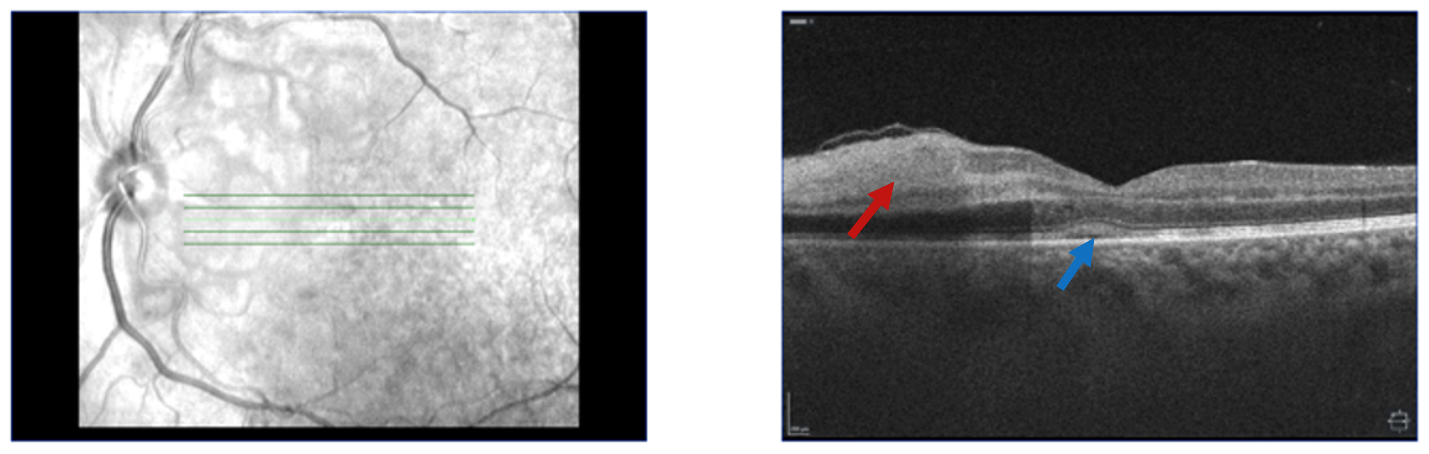
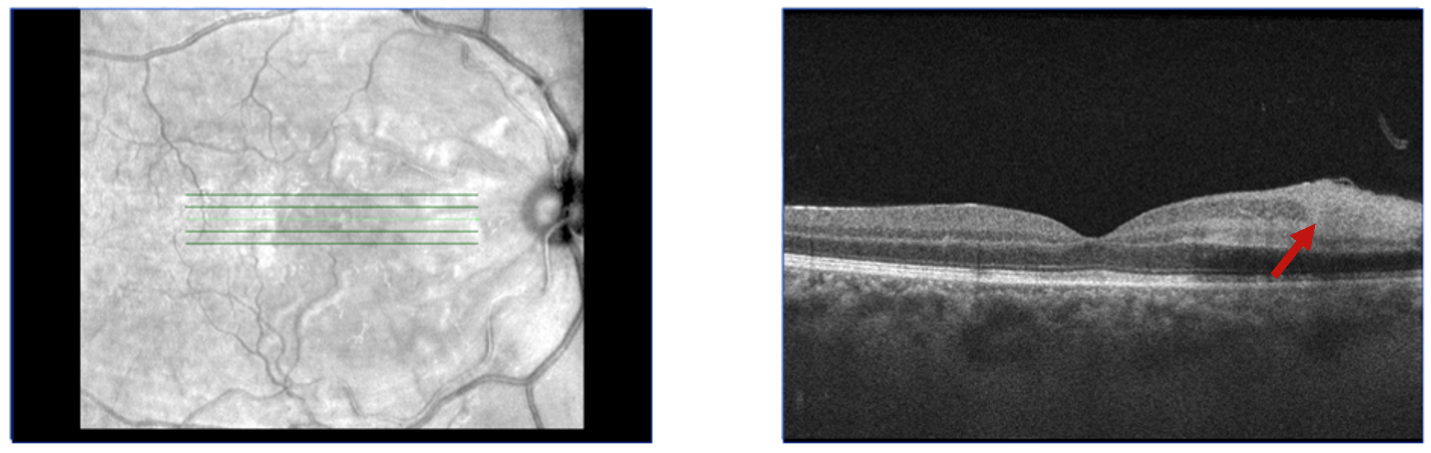
On outpatient follow up one week later, the patient was assessed by a retina specialist where she reported improvement of her visual symptoms. Her visual acuity was 20/60 on the right and 20/100 on the left. Slit lamp exam was normal OU. Fundoscopic exam revealed bilateral peripapillary and posterior pole retinal whitening consistent with Purtscher flecken along with scant inferior intraretinal hemorrhages. Ocular coherence tomography (OCT) showed inner retinal hyperreflectivity / thickening in the nasal macula and focal scant subfoveal subretinal fluid, with the left eye being more affected than the right (Figures 1 and 2). These OCT findings were consistent with acute microvascular ischemia. Decision for conservative management was made and no systemic steroids were administered, given the limited evidence of improved visual outcomes with steroid treatment, as well as the potential ocular side effects of steroid treatment including cataracts, glaucoma and ocular hypertension.8
_of_the_left_eye_horizontally_cut_at_the_level_of_the_fov.png)
_of_the_right_eye_horizontally_sliced_at_the_level_of_the.png)
The patient was subsequently followed up every 2-3 months with repeat dilated exams and OCT. She reported gradual improvement of her visual symptoms. Fundoscopic exam at 5 and 8 months after discharge revealed complete resolution of all the retinal spots, while repeat OCT demonstrated inner retinal thickening consistent with chronic retinal injury. The patient was advised that she could expect further visual improvement over the next several months, but there would likely be some permanent visual deficit.
Discussion
Purtscher-like retinopathy is a pathologic entity that can present because of several non-traumatic insults, in contrast to Purtscher retinopathy that presents following trauma. The American Academy of Ophthalmology reports several causes of this rarely identified retinopathy.9 Of these, acute pancreatitis has only been reported in 47 case reports or case series in the literature so far. Fifteen of these publications are either in a language other than English, or their full text is not available online due to being published more than 50 years ago. Among the 32 available cases, the patient age range was between 20-57 years, with half of the reported patients (16 out of 32) being around 30 (+/-5) years old (Table 1).10–40 There seems to be a significant difference between males and females, with the males being almost double in number (11 reported female patients and 20 reported male patients – sex was unavailable in one of the case reports) (Table 1). Alcohol use was the culprit for the development of pancreatitis in 22 out of the 32 cases. Other less frequent causes of pancreatitis included hypercalcemia with milk-alkali syndrome, pre-eclampsia, Klatskin tumor, drug-induced pancreatitis, or idiopathic pancreatitis (Table 1). In three cases the patients were treated with corticosteroids (1 with intravitreal injections and 2 with systemic administration).27,29,31 Most patients reported improved vision within 2-3 months, while in one of the cases the visual defects were permanent, and two of the patients died soon afterwards, hence there was no ophthalmology follow up (Table 1).16,26,38
The low reporting rate of pancreatitis-induced Purtscher-like retinopathy could be due to low incidence of this pathology in the setting of acute pancreatitis or due to the low recognition rates of the association between visual pathology and acute pancreatitis. The latter could be due to several confounding factors. First, considering that patients with acute pancreatitis usually present in the setting of alcohol intoxication/withdrawal, it is possible that they could attribute painless visual changes to alcohol use and not report them as a concern. If the responsible clinician has low suspicion for this retinal pathology, it is likely that it will be missed if a thorough history and physical examination are not obtained. Even if the visual symptoms are reported by the patient, they could be attributed by the care team to alcohol use or to potential methanol consumption. Moreover, the condition may be initially asymptomatic, therefore, when patients with resolved acute pancreatitis present with isolated retinopathy later, in the outpatient setting, this is not appropriately correlated to the preceding acute pancreatitis event.41 Finally, even when the patient reports visual symptoms and retinopathy related to acute pancreatitis is suspected, Purtscher flecken (the pathognomonic finding) may be missed on examination, especially in a non-dilated fundoscopic exam.2
There is no currently available evidence-based treatment for this retinopathy. A handful of therapeutic options have been reported so far including high-dose systemic corticosteroids, intravitreal corticosteroids, intravitreal bevacizumab, papaverine hydrochloride, hyperbaric oxygen, with outcomes that are likely not significantly different from conservative management with observation.2,27,42–45 Watchful waiting is currently the preferred management approach.2
Resolution of visual derangements is variable. Half of cases can expect spontaneous improvement of their vision by 2 Snellen lines overall.46 The visual symptoms of Purtscher-like retinopathy can be quite debilitating, further research is warranted for the development of more effective treatment options.
Funding sources
No funding sources were used for the preparation of this manuscript.
Conflict of interests
We have no conflict of interest to declare.
Consent
The patient was informed that data concerning the case would be submitted for publication, and she provided consent.
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
-
Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
-
Drafting the work or revising it critically for important intellectual content; AND
-
Final approval of the version to be published; AND
-
Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
None.
{kind=link}