In 1509, Albrecht Dürer (1471-1528) completed the paneled oil painting “Heller Altarpiece” named after its commissioner, Jakob Heller. The piece was finished with the cooperation of Matthias Grünewald (1470-1528), one of Durer’s German Renaissance confrères. The triptych depicts the coronation of the Madonna as she rises towards heaven. Surrounding her sarcophagus, the 12 apostles congregate and pray at the sight of the miracle unfolding before them. Before finishing the piece, Dürer sketched many preparatory pieces, including his most renown “Praying Hands” depicting the hands of an apostle loosely joined together. One may already know of these famed hands as Dürer’s art has permeated through today’s culture, from coffee mugs to Andy Warhol’s tombstone. Many have postulated that these hands are indicative of afflictions suffered by the owner, including Diabetes and Rheumatoid Arthritis.1 However, a better case can be made for another of his preparatory sketches.
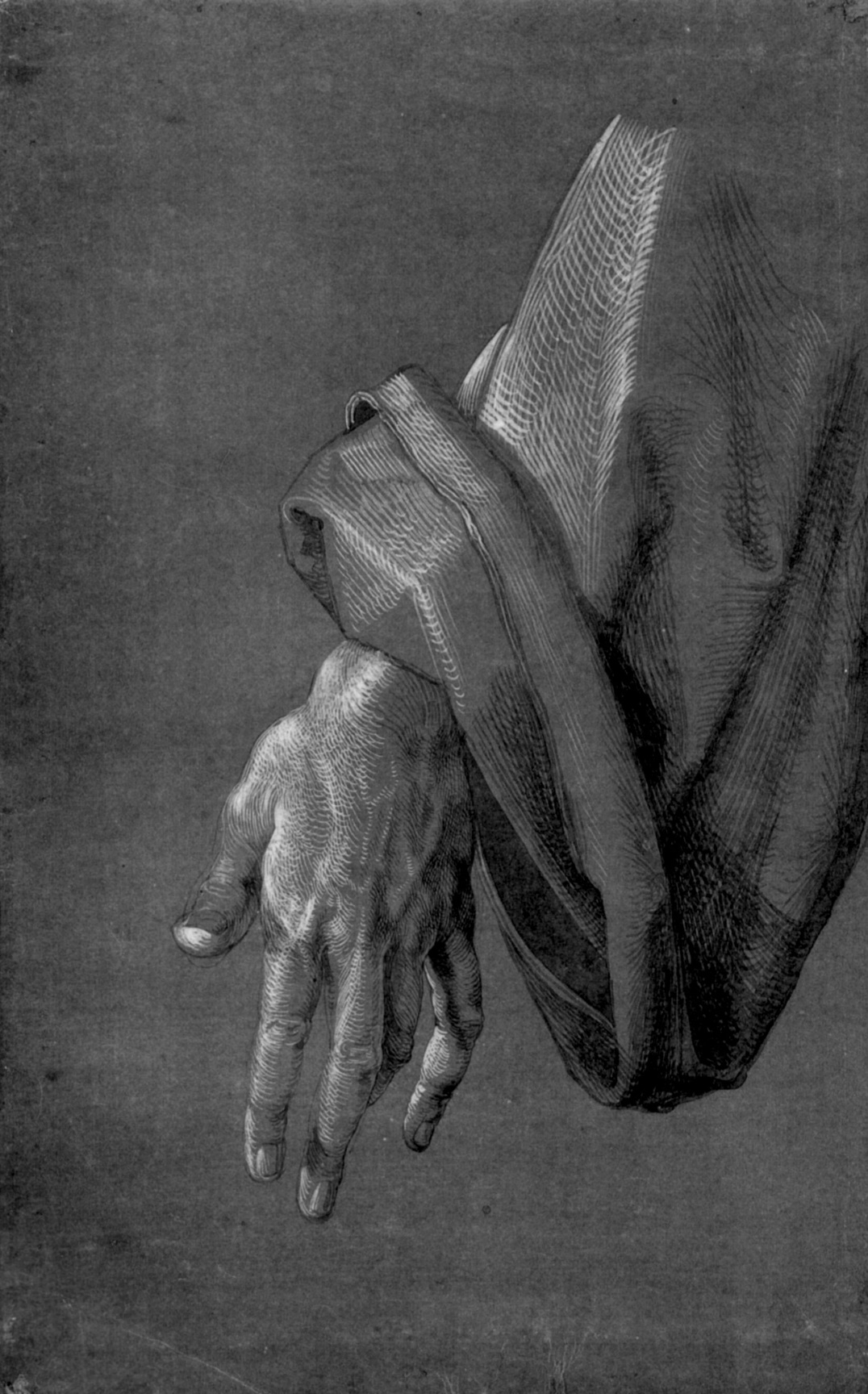
Often overlooked, the “Left Hand of an Apostle,” sketched approximately in 1508 as part of these study drawings for the altar piece, portrays the tortured left hand of yet another apostle (Figure 1).2 Although this sketch is merely a preparation for his masterpiece, Dürer’s attention to details peers out of the page through each stroke of black ink; the fingers are long and slender, the veins are full, the tendons and muscles are subtle yet realistic. Notwithstanding the intricate details of the hand, the obvious hand deformities leap out of this particular preparatory study. Both the flexion of the metacarpophalangeal joint and the extension of the distal interphalangeal joint of the thumb are apparent – more commonly referred to as Hitchhiker’s thumb (although, Dürer would certainly not, as for a well-documented lack of highways and cars in his time). The third digit shows early signs of boutonniere’s deformity, illustrated by the flexion of the proximal interphalangeal joint and extension of the distal interphalangeal joint. Although limited by our ability to obtain a history and quantify this patient’s rheumatoid factor, anti-citrullinated peptide antibodies, or C-reactive protein, the image suggests signs of rheumatoid arthritis (RA).
__*left_hand_of_an_apostle_*_1508__german._ink.jpeg)
The first clinical description of RA, however, came from France in 1800 when Augustin Jacob Landré-Beauvais (1772-1840) described symptoms closely related to RA. Landré-Beauvais went against the already established description of gout to describe a chronic condition which affects multiple joints upon onset and predominates in women. Landré-Beauvais cites the physician’s inclination towards pathologies that affected higher social classes as the main reason for RA’s lack of characterization.3 In accord with Landré-Beauvais’s point, these events recount a failure of the medical field to pay attention. Insofar as monetary incentives fueled the doctor’s attention, the evidence for RA existed long before the medical field would categorize the pathology.
How can we learn from such a lapse by the medical field in identifying sooner a pathology well illustrated by non-medical professionals. In particular, can artists’ skills and their acumen for observation be taught to young medical professionals at the onset of their careers? Over the last 20 years, formal art observation training has been studied at varying medical schools and the results are consistent: training improves the quantity and quality of observations made by medical students in response to diverse clinical scenarios.4–6 However, only a narrow number of medical schools have included workshops aimed at integrating art analysis into their curriculum and many schools have yet to hear the artists’ input. Observation skills in young medical professionals must be nurtured using the accumulated knowledge produced by the professionals of “optical realism,” especially when clinical diagnoses and research depends on being attuned to subtleties hidden in plain sight.
This situation further draws on a philosophical conversation about knowledge and how we learn. In 2002, at a NATO press conference in Brussels, Donald Rumsfeld answered a question about how situations may differ from the way facts are described through a more philosophical exercise: “There are no ‘knowns.’ There are things we know that we know. There are known unknowns. That is to say there are things that we now know we don’t know. But there are also unknown unknowns. There are things we don’t know we don’t know.” In 2008, Slovenian philosopher Slavoj Zizek, in response to Donald Rumsfeld, expanded on Rumsfeld’s theory of knowledge by adding the concept of “unknown knowns - things we don’t know that we know.”7 In this case, Dürer’s precision and penchant for details served to depict a condition that would only be characterized 300 years later. Only once Landré-Beauvais peered into the clinical features, were we able to differentiate RA from gout. For years, we knew but we were unaware of knowing. What other pathologies might art be hiding? What do we know but can’t quite grasp? In that sense, artists may help the medical field to uncover new “unknown knowns.”
Corresponding Author:
Isaac Jules Benque
533 Parnassus Ave, San Francisco 94143
Email: isaac.benque@ucsf.edu
Phone: 650-714-0496
Disclosures/Conflicts of interest
The author has no conflicts of interest to disclose.